Nationwide Pain & Injury Medical Expert Witness
Amputation & Phantom Limb Pain Expert Witness
Expert evaluation of post-amputation pain syndromes — phantom limb pain, residual limb pain, neuroma pain, causation, treatment necessity, standard of care, and future medical care in complex pain and injury-related litigation.
Request AvailabilityCredentials & Qualifications
- Conditions
- Phantom Limb Pain, Post-Amputation Pain
- Also Covers
- Residual Limb Pain, Stump Neuromas, Neuroma-Related Pain
- Specialty
- Pain Management & Anesthesiology
- Evaluation Areas
- Causation, Treatment Necessity, Standard of Care, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Post-Amputation Pain in Medical-Legal Review
Amputation — whether from traumatic injury, vascular disease, infection, or cancer — produces a distinct constellation of pain conditions that are among the most clinically complex and medico-legally significant in personal injury and malpractice litigation. These cases often involve catastrophic injury, high damages, and long-term future care projections that require a detailed understanding of pain mechanisms, treatment options, and the clinical record.
Three conditions are commonly encountered in post-amputation pain litigation and require careful differentiation:
- › Residual limb pain — Pain perceived at the physical site of amputation, in the remaining tissue. It may arise from neuroma formation at severed nerve endings, soft tissue complications, bone spurs, skin breakdown from prosthetic use, or other local pathology. Residual limb pain has peripheral generators that can often be targeted with interventional approaches.
- › Phantom limb sensation — Non-painful awareness or perception of the absent limb, including the perceived position, movement, or pressure of the missing extremity. Phantom limb sensation is extremely common following amputation and is not in itself a pain condition requiring treatment.
- › Phantom limb pain — Painful perception in the absent portion of the amputated limb. This is a distinct neuropathic pain condition arising from neural changes at both the peripheral and central levels following limb loss. It is the most clinically significant of the three conditions and the most common source of long-term pain management need.
Accurate differentiation of these conditions in the clinical record is a foundational element of expert review. Treatment approaches, cost projections, and the clinical literature differ materially between residual limb pain and phantom limb pain — and imprecise documentation that conflates them is a recurring issue in both treating records and life care plans.
What Is Phantom Limb Pain?
Phantom limb pain is neuropathic pain perceived in the absent portion of an amputated extremity. It is experienced by a majority of amputees — epidemiological studies report prevalence ranging from 50% to 80% of amputees — and may begin immediately after amputation or develop weeks to months following limb loss. Pain quality is variable: patients commonly describe burning, cramping, squeezing, stabbing, electric, or shooting sensations that may be continuous or episodic, and that may be triggered by temperature change, emotional stress, prosthetic use, or contact with the residual limb.
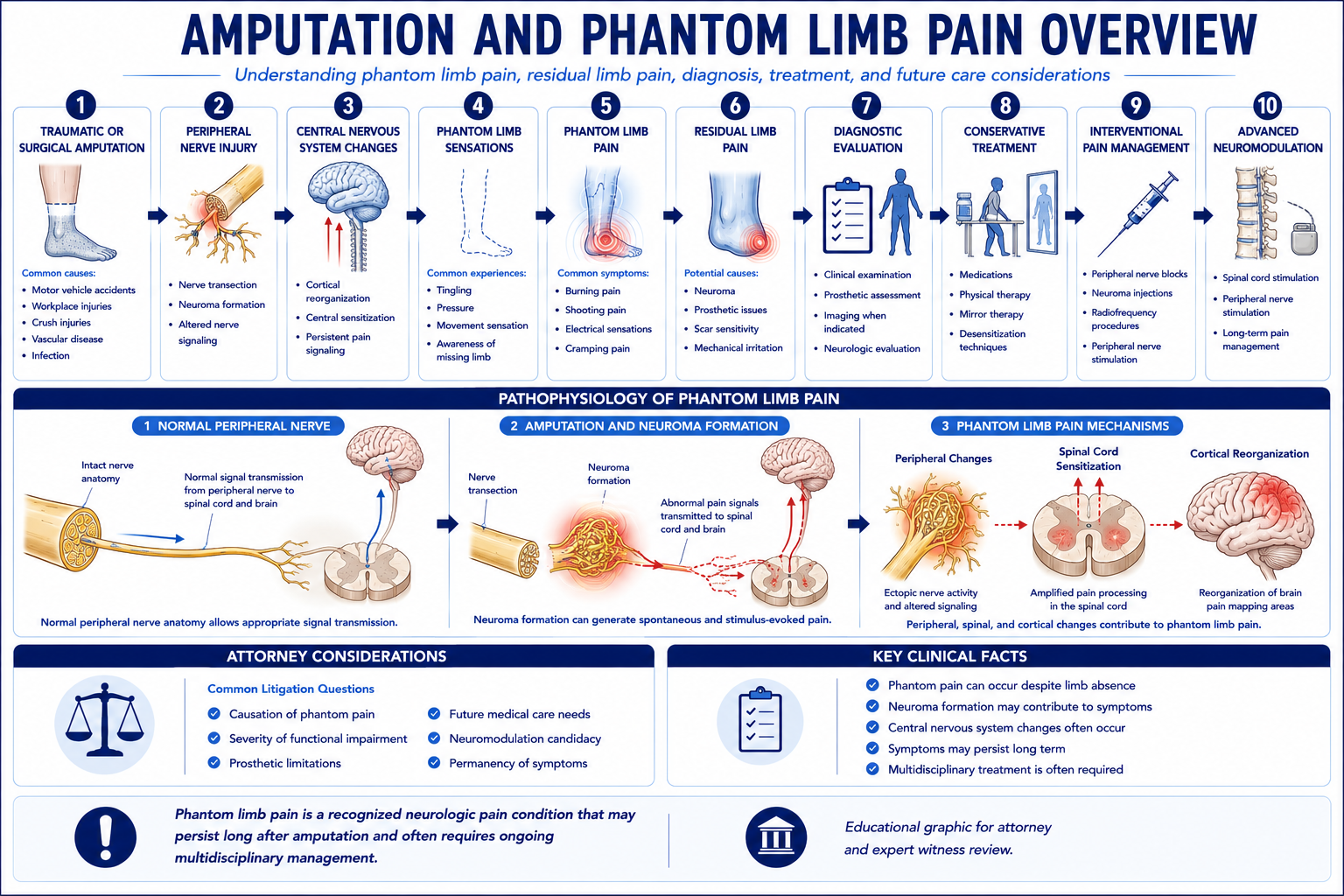
The mechanisms of phantom limb pain are multifactorial and involve both peripheral and central nervous system changes:
- › Peripheral nerve injury and neuroma formation — Amputation severs peripheral nerves, leaving proximal nerve endings that attempt to regenerate distally. Without a distal target, the regenerating axonal sprouts form disorganized neuromas at the residual limb site. Neuromas generate spontaneous and ectopic electrical discharges that contribute to both residual limb pain and phantom limb pain. The peripheral component is important because it represents a potentially targetable pain generator for interventional treatment.
- › Central sensitization — Chronic peripheral pain signals from the amputation site can induce neuroplastic changes in the dorsal horn of the spinal cord — including upregulation of NMDA receptors and loss of inhibitory interneurons — that amplify and perpetuate pain signaling even in the absence of ongoing peripheral input. Central sensitization is relevant to treatment selection because it explains why peripheral interventions alone may provide incomplete relief in chronic phantom limb pain.
- › Cortical reorganization — Following limb loss, the somatosensory cortex undergoes reorganization as cortical areas previously representing the amputated limb are invaded by neighboring representations. This cortical remapping is associated with phantom limb pain, and the degree of reorganization has been correlated with pain intensity in some studies. Cortical reorganization underlies the rationale for non-invasive treatments including mirror therapy and graded motor imagery, which aim to normalize cortical representations through visual and motor feedback.
- › Pre-amputation pain — Pre-amputation pain in the affected limb is a recognized risk factor for phantom limb pain development and intensity. Patients who experienced significant limb pain before amputation — from vascular disease, infection, neuropathy, or traumatic injury — are more likely to develop phantom limb pain and may experience it with a quality resembling the pre-amputation pain. This clinical relationship is relevant to causation analysis in cases where pre-existing limb pathology predated the event requiring amputation.
Symptom presentation varies considerably between patients. Some individuals experience severe, continuous pain that significantly impairs daily function; others experience intermittent pain episodes with preserved functional capacity. The variability in clinical presentation means that objective documentation of pain severity and functional impact in the treating records is essential to expert review of damages claims in phantom limb pain litigation.
Causes, Mechanisms, and Clinical Context
Post-amputation pain syndromes arise following both traumatic and non-traumatic amputations. The etiology of amputation is relevant to expert review because it affects causation analysis, the relationship between pre-amputation conditions and post-amputation pain, and the context in which damages are assessed.
Traumatic amputations — arising from motor vehicle collisions, motorcycle accidents, industrial and workplace accidents, crush injuries, and blast or explosive injuries — present the most direct causation pathway in personal injury litigation. The connection between the traumatic event and the need for amputation is typically established through the trauma records and operative documentation. Post-amputation pain in this context is a recognized and foreseeable consequence of the traumatic limb loss, and expert review addresses the clinical characterization of the pain syndrome, its treatment, and the projected future care needs attributable to the injury.
- › Motor vehicle collisions — Traumatic below-knee and above-knee amputations following high-energy motor vehicle and motorcycle accidents are among the most common traumatic amputation mechanisms in personal injury litigation. Crash biomechanics, injury severity scoring, and the perioperative record establish the traumatic basis for limb loss.
- › Industrial and workplace accidents — Crush injuries, entrapment, and machine-related amputations produce traumatic nerve injury at the amputation site that may be more severe than surgical amputation, with a higher rate of neuroma formation and more complex post-amputation pain presentations.
- › Non-traumatic amputations — Amputations performed for vascular disease, diabetic complications, infection, or oncological indications may be relevant in medical malpractice contexts — where the question is whether the amputation was clinically indicated and appropriately timed — or in personal injury contexts where a pre-existing condition is alleged to have contributed to an amputation that followed trauma.
- › Upper vs. lower extremity amputation — Upper extremity amputations — including digit, partial hand, transradial (below-elbow), and transhumeral (above-elbow) amputations — produce phantom limb pain with distinct characteristics and treatment considerations compared to lower extremity amputation. The phantom limb pain evaluation addresses the specific anatomy of the amputation, the nerve territories involved, and the treatment modalities appropriate to the level of limb loss.
The relationship between pre-amputation conditions and post-amputation pain is clinically important and legally relevant. Vascular insufficiency, peripheral neuropathy, prior fractures or injuries, or pre-existing limb pain at the affected extremity may influence post-amputation pain development and intensity. These pre-existing factors are part of the causation and apportionment analysis where their relevance is disputed.
Medical Necessity and Treatment Evaluation
Treatment of post-amputation pain syndromes follows a graduated approach from conservative to more invasive modalities. Expert review addresses whether the treatments rendered or proposed are consistent with recognized clinical practice for the specific pain condition documented — whether phantom limb pain, residual limb neuroma pain, or a combination of both.
Pharmacological management is typically the first line of treatment for phantom limb pain. Anticonvulsant medications (gabapentin, pregabalin) and tricyclic antidepressants have the strongest evidence base for neuropathic pain and phantom limb pain. Opioid analgesics may be used for acute and subacute post-amputation pain, with recognized limitations for long-term neuropathic pain management. The rationale for the medications prescribed, the documented response to each agent, and the clinical basis for any medication changes are reviewed in both necessity and standard of care analysis.
Non-pharmacological treatments with evidence support for phantom limb pain include mirror therapy — in which a mirror creates the visual illusion of an intact limb, reducing cortical reorganization-mediated pain — and graded motor imagery, a structured sensory and motor rehabilitation program. Physical therapy and desensitization techniques for the residual limb also form part of the standard rehabilitative approach. The availability and clinical rationale for these treatments is relevant to necessity review when they have not been recommended or completed.
Interventional approaches for residual limb neuroma pain include nerve blocks targeting the identified neuroma, peripheral nerve stimulation, targeted muscle reinnervation (TMR) as a surgical strategy to redirect regenerating axons and reduce neuroma formation, and, in appropriate cases, surgical neuroma excision with or without nerve reconstruction. The indication, timing, and expected benefit of these approaches depend on the clinical presentation and the available surgical and interventional resources.
Neuromodulation — including spinal cord stimulation — is considered for post-amputation pain refractory to conservative and conventional interventional management. Published evidence and case series support SCS for both phantom limb pain and residual limb pain that has not responded to less invasive treatment. As with other SCS indications, a formal SCS trial demonstrating adequate relief is required before permanent implantation. In high-value personal injury cases, the future cost of SCS — including trial, implantation, battery replacement, and programming — may be a significant component of the damages calculation. For a detailed discussion of SCS necessity and cost analysis, see the Spinal Cord Stimulation Expert Witness page.
Standard of Care Considerations
The standard of care for post-amputation pain management addresses the reasonable practice of a board-certified or board-eligible pain management physician evaluating and treating patients with phantom limb pain or residual limb pain syndromes. Standard of care review is case-specific — it evaluates what was done in light of what was documented, against the applicable clinical standards for the patient's presentation at the relevant time.
- › Initial evaluation and characterization — The initial pain management evaluation should document the character, location, and intensity of pain; distinguish between residual limb pain, phantom limb sensation, and phantom limb pain; assess functional impact; review the surgical and perioperative history; and address any pre-existing pain conditions at the affected extremity. Failure to differentiate the pain syndromes present may result in a treatment approach that does not address the actual clinical problem.
- › Neuroma assessment — Residual limb neuroma pain is a specific and targetable component of post-amputation pain that requires clinical identification. A standard evaluation should address whether point tenderness at the residual limb site, a Tinel's sign along a specific nerve distribution, or characteristic lancinating pain with prosthetic use suggest neuroma involvement. Failure to evaluate for and address neuroma pain in a patient with residual limb symptoms is relevant to standard of care review where neuroma-directed treatment was available and potentially beneficial.
- › Graduated treatment approach — Standard post-amputation pain management generally follows a progression from first-line pharmacological therapy and rehabilitative approaches through interventional pain procedures and, where indicated, neuromodulation. Premature escalation to high-cost or high-risk interventions without an adequate trial of less invasive treatment, or failure to escalate when conservative measures have clearly failed, are both standard of care considerations.
- › Documentation of treatment response — Contemporaneous documentation of pain intensity, functional status, and treatment response using validated outcome measures provides the clinical and evidentiary record on which expert review is based. Treating records that consist primarily of prescription refills without documented pain assessments, functional outcome measures, or clinical rationale for treatment changes provide an inadequate basis for standard of care defense and complicate expert evaluation on both sides.
- › Coordination with rehabilitation and prosthetics — Pain management for the amputee patient is most effective when integrated with the prosthetic fitting and rehabilitation program. Prosthesis-related pain — from socket fit issues, skin breakdown, or biomechanical malalignment — requires coordination between the pain management team and the prosthetist. Pain management notes that do not address the patient's prosthetic status and any prosthesis-related pain contributions reflect an incomplete evaluation.
Common Litigation Issues
Post-amputation pain cases present a defined pattern of litigation issues across personal injury and medical malpractice contexts. Understanding these patterns informs the records to gather and the questions that expert review should address.
- › Causation disputes — Whether the post-amputation pain syndrome is causally related to the subject accident or injury, or whether it is primarily attributable to pre-existing conditions, is a common focus of medical-legal dispute. Pre-existing vascular disease, peripheral neuropathy, prior limb injuries, and pre-amputation pain history are assessed in the causation analysis alongside the mechanism of the traumatic event.
- › Pain severity disputes — Phantom limb pain is subjective in nature, and its severity is not confirmed by imaging or laboratory findings. The clinical record — the consistency of pain complaints across treating providers, the functional documentation, the treatment response, and the medications prescribed — provides the objective evidence base for pain severity assessment. Inconsistencies in the treating record, or a clinical course in which severe pain is reported but functional limitations are not documented, may be the subject of expert comment.
- › Functional limitation disputes — The functional impact of phantom limb and residual limb pain — on ambulation, prosthetic tolerance, vocational capacity, and daily activities — is frequently contested. Expert review addresses whether the functional limitations documented in the record are consistent with the clinical findings and the pain condition described, and whether the treating record adequately documents functional status over time.
- › Future treatment projection disputes — Life care plans and future medical care projections for amputee patients frequently include pain management components that are subject to expert challenge. Common disputes address the clinical basis for proposed neuromodulation, the projected frequency and cost of interventional procedures, the duration of need for pharmacological management, and whether proposed items reflect the current standard of practice or speculative future therapies.
- › CRPS Type II following amputation-related nerve injury — In cases where traumatic amputation was associated with significant nerve injury, the possibility that the peripheral nerve injury produced CRPS Type II (causalgia) in addition to or separately from phantom limb pain may arise. CRPS Type II requires a confirmed peripheral nerve injury and produces a clinical syndrome overlapping with but distinct from standard phantom limb pain. Its presence affects both the diagnosis and the future care analysis.
- › Neuroma identification and treatment disputes — Neuromas that are identifiable by examination and potentially amenable to targeted treatment represent a distinct clinical opportunity. In cases where residual limb neuroma pain has not been specifically evaluated or addressed, expert review may address whether a neuroma evaluation was part of the standard workup and whether neuroma-directed treatment was considered or available.
Personal Injury Case Analysis
Traumatic amputation cases are among the highest-value personal injury matters — and the pain management dimensions of these cases are often the most complex to address. The physical loss of a limb is straightforward to document; the nature, severity, and long-term trajectory of the associated pain syndromes requires a pain management specialist to evaluate against the clinical record.
Mechanism of injury and causal pathway — Expert review of the mechanism of injury establishes the biomechanical basis for both the traumatic limb loss and the severity of associated nerve injury. High-energy trauma, crush mechanisms, and blast injuries produce greater peripheral nerve damage at the amputation site than surgical amputations — which has implications for neuroma formation rates, phantom limb pain severity, and treatment needs. The perioperative and surgical records document the level of amputation, the nerve handling technique employed, and any complications identified at the time of surgery. In cases involving high-energy polytrauma — blast injuries, high-speed collisions, and catastrophic industrial mechanisms — traumatic amputation may occur alongside spinal injury severe enough to cause cauda equina syndrome, requiring the pain management evaluation to address both the post-amputation pain syndrome and the distinct neuropathic sequelae of cauda equina nerve root compression as separate components of the damages analysis.
Temporal relationship and treatment chronology — The development of phantom limb pain following amputation follows a recognized but variable timeline. Pain may begin in the acute postoperative period or develop over weeks to months following limb loss. The treating record should document when pain was first reported, how it was characterized at the time, and how the clinical picture evolved. Gaps in the record, delayed initial presentation to pain management, or significant inconsistencies in reported symptoms over time are relevant to the assessment of pain chronology and severity.
Pre-existing conditions and apportionment — In cases involving pre-existing peripheral vascular disease, diabetic neuropathy, prior injury to the affected extremity, or prior pain conditions, the causation analysis must address the contribution of pre-existing conditions to the post-amputation pain syndrome. A person with pre-existing peripheral neuropathy who undergoes traumatic amputation may have a more severe phantom limb pain course than a neurologically intact individual — but the traumatic event remains the proximate cause of the limb loss and the consequent pain syndrome. Expert review addresses this analysis on the specific facts of the case without applying predetermined conclusions.
Functional impact documentation — Objective documentation of functional status in the treating records — including prosthetic tolerance and wear time, ambulatory capacity, reported activity limitations, and psychological status — provides the factual foundation for damages assessment. Functional capacity evaluations, physical therapy progress notes, and rehabilitation records are important supplements to the pain management record in establishing the functional impact of the pain syndrome over time.
Future Medical Care Considerations
Future medical care for post-amputation pain syndromes represents one of the most complex components of life care planning in catastrophic injury cases. The pain management component of a comprehensive life care plan must be grounded in the documented clinical course, the current treatment status, and the recognized natural history of the specific pain syndrome — and must account for the evolving nature of both the pain condition and the prosthetic interface over time.
Pharmacological management — Ongoing pain medication management is a recognized long-term cost for patients with chronic phantom limb pain. The projected medication regimen should reflect the medications currently being used with documented benefit, their established dosing, and the current cost of each agent. Speculative projections of future medications not yet prescribed or not supported by the current treatment course are subject to expert challenge.
- › Interventional procedures for residual limb pain — Patients with identified neuroma pain or prosthetic-related residual limb pain may require periodic nerve block procedures, peripheral nerve stimulation adjustments, or surgical revision. The frequency and cost of these interventions should be based on the documented treatment history and the treating physician's recommendations, not on generic life care plan templates.
- › Neuromodulation — Where spinal cord stimulation is proposed as future care based on the clinical trajectory, the projection should document: the clinical basis for the recommendation (refractory pain despite adequate conservative management); the required trial and implantation cost components; the projected battery replacement schedule based on the device type; revision procedure allowances consistent with published literature complication rates; and ongoing programming visit costs. Future SCS projections that are included without clinical support for the indication — or that omit device type specification and replacement cost documentation — are subject to both clinical and economic challenge.
- › Pain management coordination with prosthetic revisions — Prosthetic revisions — required as the residual limb matures and changes shape over the years following amputation — can alter the pain interface and produce new pain management needs. Future care projections should account for the recognized relationship between prosthetic revisions and pain management access, particularly in patients with established residual limb pain that is sensitive to socket fit changes.
- › Psychological pain management — Psychological comorbidities — including depression, post-traumatic stress disorder, and anxiety — are recognized sequelae of traumatic amputation and chronic pain, and may require ongoing psychological pain management as part of a comprehensive treatment plan. Expert review addresses whether psychological pain management is clinically supported by the documented record and whether its inclusion in a future care plan is appropriate.
Future medical care review for post-amputation pain cases can be structured as a standalone engagement or integrated with causation analysis. Contact Expert Medical Services LLC to discuss scope and available records.
Medical-Legal Record Review
Post-amputation pain cases involve a broader range of record categories than most other pain management matters, reflecting the multidisciplinary treatment pathway from traumatic injury through amputation, rehabilitation, and long-term pain management. A complete record set for expert review typically includes records from multiple treating specialties across an extended timeline.
- › Trauma and emergency records — Emergency department records, trauma surgery notes, and initial hospitalization records documenting the mechanism of injury, the severity of limb trauma, and the basis for the decision to amputate
- › Operative reports — Surgical reports documenting the level of amputation, the technique employed for nerve handling (including whether traction neurectomy or other methods were used), residual limb shaping, and any intraoperative complications
- › Perioperative and surgical follow-up records — Post-surgical wound care, residual limb healing documentation, identification of early complications, and the transition to rehabilitation and prosthetic fitting
- › Rehabilitation and physical therapy records — Inpatient and outpatient rehabilitation documentation addressing functional recovery, prosthetic training, gait training, and functional capacity documentation over the rehabilitation course
- › Prosthetic records — Initial fitting, socket adjustments, prosthetic revision documentation, and prosthetic-related complaints that may indicate residual limb pain or skin breakdown contributing to pain
- › Pain management records — Complete treating pain management notes from initial referral through the most recent encounter, including pain characterization, functional assessments, medication management, and any procedural interventions
- › Imaging studies — Imaging of the residual limb (X-ray, MRI, or ultrasound) to evaluate bone spur formation, soft tissue pathology, or neuroma identification; spinal imaging where radicular or central pain components are at issue
- › Psychological and psychiatric records — Psychological evaluation for SCS candidacy where applicable; treatment records for depression, PTSD, or anxiety; and any pre-existing psychological conditions documented before the injury
- › Prior treating records — Records predating the amputation documenting baseline health status, pre-existing vascular or neurological conditions, prior injuries to the affected extremity, and any pre-amputation pain history
Causation analysis and future medical care projections can be addressed together or structured as separate engagements depending on the questions to be resolved. For California-specific matters, see the California Pain Management Expert Witness page.
Expert Witness Review Process
Expert review in post-amputation pain matters begins with a structured chronological review of the complete medical record — from the precipitating event or onset of the condition requiring amputation through the current treatment status. The chronology establishes the factual foundation for all subsequent opinion work and identifies gaps, inconsistencies, or questions that require follow-up. For the objective evaluation methodology — examination, validated instruments, functional capacity, and symptom validity assessment — used in pain management expert review of functional impairment and treatment necessity, see the article on how pain management experts objectively evaluate pain.
The scope of opinions rendered depends on the questions defined by retaining counsel at engagement initiation. Common opinion areas include:
- › Diagnosis characterization — Whether the clinical record supports the pain diagnoses described — including the distinction between residual limb pain, phantom limb pain, neuroma pain, and any co-occurring conditions such as CRPS — and whether the documentation is adequate to substantiate those diagnoses
- › Causation analysis — Whether the post-amputation pain syndrome is supported by the record as causally related to the subject event, and whether pre-existing conditions are relevant to the causation or apportionment analysis
- › Treatment necessity and standard of care — Whether the treatment rendered to date was consistent with the applicable standard of care for the documented conditions, and whether proposed future treatment is clinically supported by the record
- › Future medical care — Identification of the pain management components of future care that are clinically supported by the record, their projected frequency and duration, and their consistency with current market costs in the plaintiff's geographic treatment area
- › Life care plan review — Defense or plaintiff review of an existing life care plan for the pain management components, addressing whether each proposed item is clinically supported by the documented record, appropriately characterized, and consistent with current clinical practice and pricing
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. The engagement scope is defined at initiation — causation, necessity, standard of care, future care, or life care plan review can be addressed together or separately.
Related Services & Expertise
CRPS Expert Witness
CRPS Type II may follow nerve injury from traumatic amputation — diagnosis, causation, and future care.
Peripheral Nerve Injury
Expert evaluation of traumatic neuropathy, neuroma formation, and electrodiagnostic findings in complex litigation.
Spinal Cord Stimulation
SCS is a recognized treatment for refractory phantom limb and residual limb pain — necessity and cost projections.
Future Medical Care Review
Long-term cost projections for post-amputation pain management, neuromodulation, and prosthetic-related care.
Causation Analysis
Linking traumatic amputation and mechanism of injury to post-amputation pain syndromes.
Medial Branch Block
Expert review of MBB medical necessity and the diagnostic pathway to RFA for concurrent spinal pain.
Radiofrequency Ablation
Expert review of RFA for facet-mediated spinal pain that may coexist with post-amputation pain conditions.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California amputation pain matters.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for phantom limb and residual limb pain treatment, including neuromodulation candidacy.
Standard of Care Analysis
Standard of care analysis for post-amputation pain management and neuromodulation in catastrophic injury cases.
FAQ
Amputation & Phantom Limb Pain — Common Attorney Questions
- Phantom limb pain is neuropathic pain perceived in the absent portion of an amputated limb. It is distinct from both phantom limb sensation (non-painful awareness of the missing limb) and residual limb pain (pain at the amputation site itself). Phantom limb pain arises from peripheral and central neural changes following amputation — including neuroma formation at severed nerve endings, altered sensory processing in the dorsal horn of the spinal cord, and cortical reorganization in the sensorimotor cortex. Pain may be perceived as burning, cramping, stabbing, electric, or shooting in quality, and may occur continuously or episodically. Phantom limb pain is a recognized chronic pain condition and can significantly affect long-term functional capacity and quality of life.
- Residual limb pain — historically called stump pain — is pain perceived at the physical site of the amputation, in the tissue that remains following the surgical procedure. It may arise from neuroma formation at severed nerve endings, skin breakdown or pressure sores related to prosthetic fitting, bone spur formation, soft tissue pathology, or infection at the residual limb site. Phantom limb pain, by contrast, is perceived in the portion of the limb that no longer exists. The two conditions are clinically distinct, may coexist in the same patient, have different treatment approaches, and are separately evaluated in medical-legal review. Accurate characterization of which pain syndrome is present — or whether both are — is a foundational step in expert record review.
- Neuroma formation occurs when a peripheral nerve is severed during amputation. The proximal nerve ending attempts to regenerate but, without a distal target, forms a disorganized mass of axonal sprouts called a neuroma. Neuromas are mechanically sensitive and can generate spontaneous electrical discharges — producing severe lancinating or burning pain in the residual limb that is often exacerbated by prosthetic use, contact, and pressure. Neuroma pain is a specific and often underrecognized component of residual limb pain. Expert review addresses whether the clinical record documents a neuroma evaluation, whether neuroma-directed treatment was considered or applied, and whether neuroma pain is a distinct component of the patient's pain syndrome requiring separate future care planning.
- Causation review in amputation pain litigation addresses two levels of analysis. First, whether the subject event — traumatic accident, medical complication, or other precipitating cause — produced the conditions requiring amputation. Second, whether the post-amputation pain syndrome (phantom limb pain, residual limb pain, or neuroma pain) is a recognized sequela of the amputation itself. Phantom limb pain and residual limb pain are well-documented sequelae of limb loss, and the causation analysis in traumatic amputation cases generally addresses the former question rather than contesting the latter. Pre-existing conditions, vascular disease, prior injuries to the affected extremity, and pre-amputation pain history are relevant to causation and apportionment where applicable.
- Functional limitations in post-amputation pain cases may include impaired prosthetic tolerance (pain that limits prosthetic use, reducing ambulation and activity), sleep disturbance from phantom pain episodes, difficulty with vocational activities requiring standing, walking, or use of the affected extremity, and psychological sequelae including depression and anxiety that are recognized comorbidities of chronic post-amputation pain. Expert review addresses whether the functional limitations documented in the clinical record are consistent with the pain syndrome described, whether they are supported by objective findings, and whether the treatment rendered to date has addressed functional restoration as well as pain control.
- Spinal cord stimulation is considered for post-amputation pain when the condition is refractory to conservative and conventional interventional management — including pharmacological treatment with neuropathic agents, mirror therapy, peripheral nerve blocks, and other modalities. Published evidence and case series support SCS for both phantom limb pain and residual limb pain that has not responded to less invasive approaches. As with all SCS indications, a formal SCS trial demonstrating adequate pain relief is required before permanent implantation. Future medical care projections in high-value amputation cases may include SCS trial and implantation costs, battery replacement cycles, and ongoing device management.
- Long-term future care for post-amputation pain syndromes may include ongoing pharmacological management with neuropathic pain agents; periodic procedural interventions for neuroma pain or residual limb pathology; neuromodulation therapies including spinal cord stimulation where indicated; prosthetic-related pain management as prosthetic fitting and revision needs evolve; psychological pain management; and physical and occupational therapy for functional rehabilitation. Future care projections are case-specific and are grounded in the documented clinical course, the current treatment status, and the recognized natural history and treatment literature for the specific pain syndrome. The aggregate cost of long-term post-amputation pain management can be substantial and is a recognized component of damages in catastrophic injury cases.
- Key records include: the operative report(s) documenting the amputation procedure and surgical findings; trauma records and emergency department records from the precipitating event; vascular surgery, orthopedic, or surgical follow-up records addressing residual limb care and healing; prosthetic records documenting fitting, adjustments, and any prosthesis-related complications; pain management records from initial referral through current treatment; imaging studies of the residual limb and relevant spinal levels; rehabilitation and physical therapy records; psychological evaluation records; prior treating records predating the amputation to establish baseline; and billing records where cost is at issue.
- Yes. Dr. Dardashti accepts post-amputation pain engagements for both plaintiff and defense counsel, as well as insurance defense and medical malpractice matters for both sides. Review is available for causation analysis, treatment necessity and standard of care review, and future medical care projections — or for a defined subset of those issues based on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain Dr. Dardashti for an Amputation Pain Case
Dr. Dardashti accepts post-amputation pain engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.