Nationwide Pain & Injury Medical Expert Witness
Medial Branch Block Expert Witness: Medical Necessity, Standard of Care, and Litigation Review
Expert evaluation of medial branch blocks in personal injury and medical malpractice — medical necessity, standard of care, causation, and the diagnostic pathway to radiofrequency ablation.
Request AvailabilityCredentials & Qualifications
- Topic
- Medial Branch Block (MBB)
- Also Known As
- Facet Joint Nerve Block, Zygapophyseal Nerve Block
- Specialty
- Interventional Pain Management
- Evaluation Areas
- Medical Necessity, Standard of Care, Causation
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Medial Branch Blocks in Litigation
Medial branch blocks are among the most frequently performed interventional pain procedures in clinical practice — and among the most frequently scrutinized in personal injury and medical malpractice litigation. Their dual role as both a diagnostic tool and a therapeutic intervention, combined with the high volume at which they are performed and billed, makes them a recurring subject of medical necessity disputes, standard of care review, and causation analysis.
Litigation involving medial branch blocks commonly raises questions about whether the procedure was clinically indicated, whether it was performed within the applicable standard of care, whether the number of procedures was appropriate, and whether the decision to proceed to radiofrequency ablation was properly supported by diagnostic findings. In personal injury matters, additional questions arise about whether facet-mediated pain was caused or aggravated by the subject event.
What Is a Medial Branch Block?
Facet joints — also called zygapophyseal joints — are paired synovial joints located at each vertebral level along the posterior spine. They provide stability, guide range of motion, and can become a significant source of axial pain following injury, degeneration, or inflammatory change. Each facet joint receives sensory innervation from the medial branch nerves, which are small rami of the posterior primary divisions of the spinal nerve roots. Because of this dual innervation pattern, blocking the medial branch nerves at two consecutive levels is required to fully anesthetize a single facet joint.
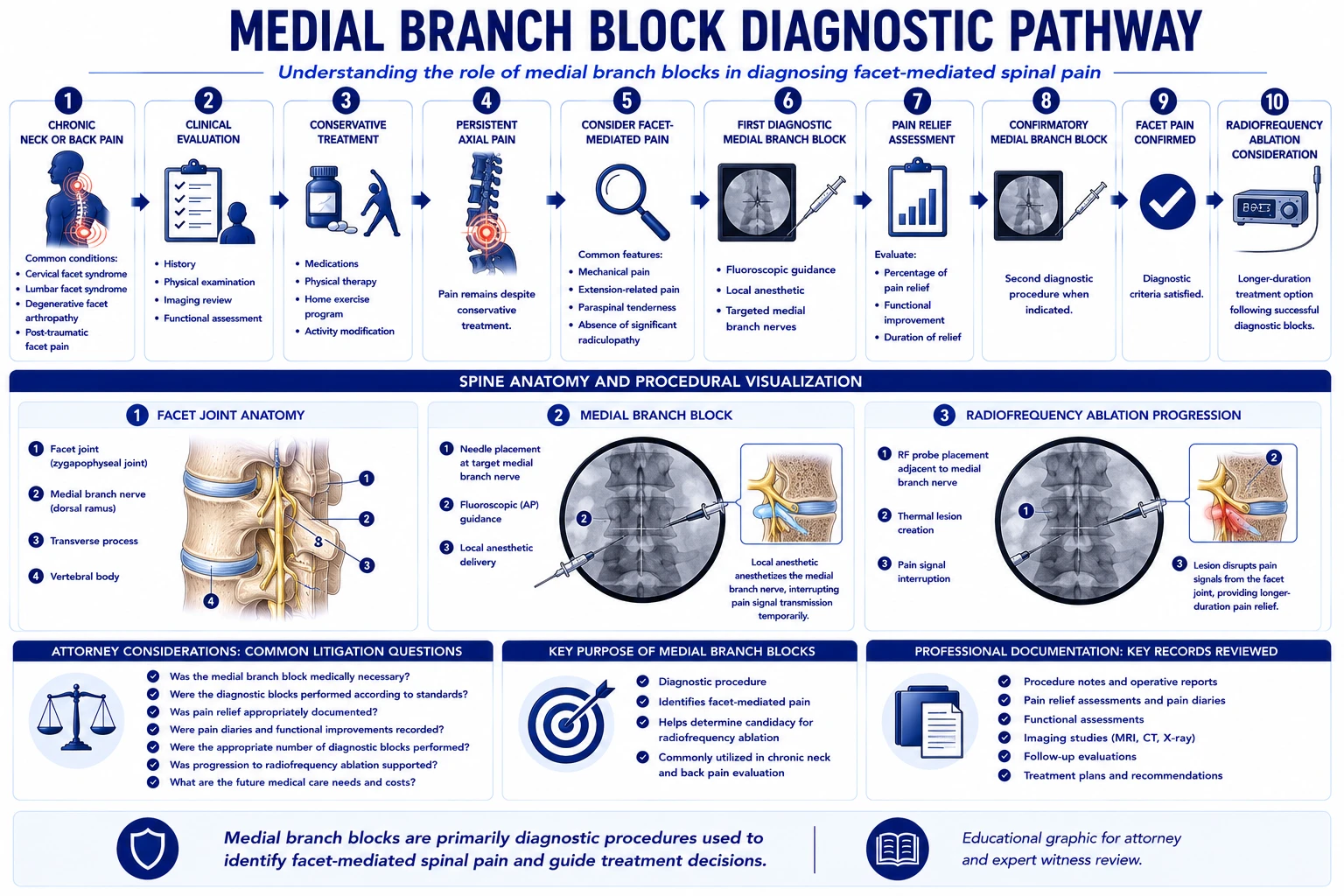
A medial branch block is a fluoroscopically guided injection of local anesthetic — with or without a small volume of corticosteroid — onto the medial branch nerves supplying the target facet joint. By temporarily interrupting the pain signal from those nerves, the procedure evaluates whether the facet joint is a clinically significant pain generator. When the anesthetic produces measurable pain relief, the result supports a facet-mediated pain diagnosis and informs the subsequent treatment pathway.
In the cervical spine, medial branch blocks address facet-mediated neck pain, cervicogenic headache, and referred pain patterns to the shoulder and upper extremity that do not involve nerve root compression. Cervical facet levels C2–3 through C6–7 are the most commonly implicated in post-traumatic cervical pain. In the lumbar spine, medial branch blocks address axial low back pain with characteristic referred patterns to the gluteal region and proximal lower extremity that are distinct from radicular pain. Lumbar levels L3–4, L4–5, and L5–S1 are the most frequently treated in the clinical and litigation context.
Medial branch blocks serve two clinical purposes. As a diagnostic tool, they establish whether a specific facet level is the pain generator and provide the confirmatory data required before proceeding to radiofrequency ablation. As a therapeutic tool, they may provide temporary symptomatic relief during the evaluation and conservative treatment phase of a pain management plan. The distinction between diagnostic and therapeutic intent matters in the litigation context because it affects the standard of documentation required, the clinical rationale for repeated procedures, and the pathway to further interventional care.
The Diagnostic Pathway to Radiofrequency Ablation
Radiofrequency ablation uses a heat lesion to interrupt the medial branch nerve's ability to transmit pain signals from the facet joint, producing longer-duration relief than a diagnostic block. Because RFA creates a semi-permanent effect on the nerve, clinical guidelines and most payer policies require that two separate positive medial branch blocks precede any RFA procedure at the same level. This confirmatory requirement exists to verify that the pain source is accurately identified before a more definitive intervention is performed.
A positive diagnostic response is defined as a specified percentage reduction in targeted axial pain — typically at least 50% improvement, with some guidelines requiring 80% — lasting for the expected duration of the local anesthetic agent used. Short-acting agents such as lidocaine are expected to produce relief for one to four hours. Longer-acting agents such as bupivacaine are expected to produce relief for four to eight hours or longer. To account for placebo response, some protocols require that the two confirmatory blocks use different local anesthetic agents, with the duration of relief correlating to the pharmacokinetic profile of the agent used in each block.
The documentation of each confirmatory block is critical. The procedure record should specify the targeted levels, the agents and volumes used, and the patient-reported percentage of pain improvement at defined time intervals following the procedure. This contemporaneous documentation is the evidentiary basis for authorizing RFA and is frequently the subject of medical necessity reviews, insurance disputes, and standard of care litigation.
When RFA has been performed or is proposed as future care following medial branch blocks, the adequacy of the preceding diagnostic workup — the number of blocks performed, the documentation of relief, and the clinical rationale for the level or levels selected — is a central element of expert review. Because medial branch nerves regenerate over time, typically within six to twelve months, serial RFA procedures at regular intervals may become a component of future medical care projections in personal injury damages analysis.
Medical Necessity Considerations
Medical necessity for medial branch blocks is evaluated against the clinical record and applicable treatment guidelines. A supported indication generally includes documented axial spine pain consistent with a facet-mediated pattern, physical examination findings compatible with the proposed diagnosis, and a clinical course in which conservative management has not provided adequate resolution. Imaging findings at the proposed levels support the clinical rationale but are not independently diagnostic of facet-mediated pain.
Key clinical factors in necessity review include whether the pain pattern on examination corresponds to the anatomical distribution of the targeted nerves, whether the documentation of conservative treatment is adequate to support escalation to an interventional approach, and whether the proposed treatment levels are consistent with the clinical and imaging findings. Absence of documented conservative care, premature progression to interventional procedures without an adequate conservative trial, or performance of blocks at levels not supported by clinical findings are recurring medical necessity issues.
In personal injury matters, the presence of pre-existing degenerative changes in the cervical or lumbar spine does not preclude medical necessity for medial branch blocks related to a new injury or aggravation. However, the treating physician's documentation should address the relationship between the subject event, the onset or worsening of symptoms, and the clinical basis for the selected procedure and levels. The distinction between degenerative changes that pre-existed the injury and pain causally related to the event is a frequent focus of causation analysis.
The timing of medial branch blocks relative to injury is also relevant. Facet-mediated pain from acute injury may resolve with conservative treatment, and interventional procedures performed very early in the post-injury course — before an adequate conservative trial — are subject to medical necessity scrutiny. Conversely, delayed treatment with persistent documentation of axial pain unresponsive to physical therapy and analgesic management generally supports necessity. The adequacy of the conservative treatment record is a threshold issue in most insurance necessity reviews. For the physician examination methodology — including range-of-motion assessment, palpation findings, and functional documentation — that establishes the objective clinical basis for facet-mediated pain, see the article on how pain management experts objectively evaluate pain.
Standard of Care Considerations
The standard of care for medial branch blocks reflects the practice of a reasonably competent board-certified or board-eligible pain management physician performing the procedure in accordance with current professional guidelines. Core elements include appropriate patient selection based on clinical evaluation, use of fluoroscopic guidance for accurate needle placement and contrast verification, contemporaneous documentation of procedure performance and patient response, and informed consent addressing the purpose, risks, alternatives, and the diagnostic implications of the result.
- › Fluoroscopic guidance — Medial branch blocks performed without fluoroscopy cannot reliably target the medial branch nerve at the anatomically defined position on the lateral aspect of the superior articular process. Image guidance is standard of care and is required by most payers as a condition of coverage.
- › Contrast confirmation — Injection of a small volume of contrast under live fluoroscopy confirms appropriate needle position and identifies potential intravascular placement before the anesthetic is delivered. Omission of contrast confirmation is relevant to standard of care review in cases involving intravascular injection complications.
- › Diagnostic documentation — Contemporaneous documentation of post-procedure pain relief — including the percentage improvement and duration — is required to support the diagnostic interpretation of the block and to establish the clinical basis for subsequent procedures. Absent or retrospective documentation is a recurring standard of care issue.
- › Confirmatory protocol before RFA — Proceeding to radiofrequency ablation without two documented positive confirmatory medial branch blocks deviates from standard clinical practice and from the coverage criteria of most payers. The adequacy of the preceding diagnostic blocks is a central issue in RFA-related malpractice and necessity disputes.
- › Appropriate procedure frequency — The number of medial branch blocks performed should be clinically justified by the diagnostic and therapeutic purpose at each encounter. Repeated blocks without documented benefit, or blocks performed primarily to satisfy payer criteria without genuine diagnostic intent, may raise both standard of care and billing concerns.
- › Follow-up clinical evaluation — Assessment of the patient's response after each block — documenting the percentage and duration of relief and the basis for continued treatment or progression to ablation — is both a standard of care expectation and the evidentiary foundation for any subsequent procedure authorization.
Common Litigation Issues
Medial branch block cases present a recurring set of litigation issues that arise in both personal injury and medical malpractice contexts. Understanding these patterns informs the records to gather and the specific questions that expert review should address.
- › Excessive procedures without documented benefit — Multiple medial branch blocks with no contemporaneous documentation of pain relief percentage or duration, or with documented minimal response, raise both medical necessity and standard of care questions.
- › Improper progression to RFA — Radiofrequency ablation performed without two documented positive confirmatory blocks, or where the documentation does not meet the required response criteria, is a frequent source of malpractice and insurance dispute claims.
- › Documentation deficiencies — Incomplete procedure records — missing post-procedure pain assessment, absent fluoroscopy documentation, or failure to specify the levels treated — compromise the clinical and legal defensibility of the treatment course.
- › Billing and upcoding disputes — Medial branch blocks are billed per level. Treatment of multiple levels simultaneously generates higher reimbursement. Disputes arise when the number of levels billed is not supported by clinical documentation or when billing does not reflect what the procedure report describes.
- › Medical necessity disputes with payers — Insurers may dispute necessity based on absence of adequate conservative treatment documentation, failure to meet clinical criteria, or the volume of procedures performed within a defined period.
- › Causation disputes — Whether facet-mediated pain arose from the subject accident, aggravated a pre-existing condition, or was unrelated to the claimed injury is a central question in personal injury matters involving MBB treatment.
- › Pre-existing degeneration — Facet arthrosis and joint hypertrophy are common degenerative findings that may predate a traumatic event. Their presence does not establish that the treatment was unrelated to the injury, but it requires careful analysis of the pre-accident baseline and the clinical changes documented after the event.
- › Procedural complications — Adverse events including intravascular injection, infection, nerve injury, or inadvertent epidural spread may be the basis for malpractice claims where they resulted from a deviation from the standard of care.
Personal Injury Case Analysis
Motor vehicle collisions are the most common cause of traumatic facet joint injury in the personal injury context. Rear-impact collisions generate a hyperextension-flexion mechanism — whiplash — that places significant mechanical stress on the cervical facet joints, capsular ligaments, and periarticular structures. Cervical facet pain is among the most well-documented persistent pain syndromes following whiplash-mechanism injuries and is a recognized cause of chronic axial neck pain, cervicogenic headache, and referred shoulder pain. Post-mortem and fluoroscopic imaging studies have demonstrated capsular tears and hemorrhage in facet joints of individuals who sustained rear-impact collisions at speeds producing minimal vehicle damage.
In lumbar spine injury claims, axial loading, rotational forces, and direct impact can produce lumbar facet capsule injury or aggravate pre-existing facet arthrosis. Lumbar facet pain from a traumatic mechanism typically presents as axial low back pain with characteristic referred patterns to the gluteal region, hip, and proximal thigh, distinguishable from dermatomal radiculopathy by the absence of radiating leg pain below the knee and by findings on clinical examination.
Causation review in personal injury matters addresses: the temporal relationship between the accident and the onset of documented axial pain; the consistency of the pain pattern with facet-mediated origin at the proposed levels; the mechanism of injury and its anatomical plausibility; the pre-accident medical history and imaging findings; and the clinical course from injury through treatment. Expert causation analysis evaluates whether the available clinical record supports or does not support the claimed relationship between the accident and the need for interventional treatment — it does not presuppose an outcome.
When facet-mediated pain does not resolve following medial branch blocks and radiofrequency ablation, further escalation of care — including the possibility of spinal cord stimulation for refractory axial pain, or management of central sensitization that has developed in the setting of chronic facet pain — may become a future care issue in high-value personal injury matters. Documenting the trajectory of treatment and the basis for each escalation decision is relevant to both damages analysis and expert review.
Medical Malpractice Analysis
Malpractice claims involving medial branch blocks generally arise from procedural complications, improper patient selection, inadequate documentation, or failure to adhere to the diagnostic protocol required before proceeding to ablative therapy. Expert review addresses whether the care provided by the treating pain management physician met the applicable standard.
- › Intravascular injection — Injection of local anesthetic into a vascular structure can cause systemic local anesthetic toxicity with cardiovascular and neurological consequences. The use of fluoroscopic guidance with live contrast confirmation and pre-injection aspiration are standard precautions. Claims involving intravascular injection center on whether these precautions were taken and documented.
- › Infection — Procedural infection following medial branch block is rare but can result in serious outcomes including epidural abscess or facet joint septic arthritis. Claims addressing infection focus on sterile technique, skin preparation, and whether post-procedure infectious signs and symptoms were recognized and managed appropriately.
- › Nerve injury — Direct needle trauma to the exiting nerve root or spinal cord is a potential complication of incorrectly positioned injections. Fluoroscopic guidance with careful incremental needle advancement is the standard precaution against this risk.
- › Inadvertent epidural or subarachnoid spread — Injection at excessive depth or with excessive volume can produce unintended spread of local anesthetic into the epidural or subarachnoid space, with associated hypotension, motor block, and potentially more serious neurological consequences.
- › Unnecessary procedures — Performing medial branch blocks without clinical indication, continuing procedures in the absence of documented benefit, or performing RFA without adequate diagnostic confirmation may form the basis of a claim for unnecessary treatment with associated damages.
- › Documentation deficiencies as evidence of substandard practice — In some circumstances, the systematic absence of standard documentation — no pre-procedure evaluation, no fluoroscopy records, no post-procedure response assessment — may support an inference of substandard care practice separate from the documentation deficiency itself.
Expert review is within the scope of pain management and anesthesiology. Opinions on neurosurgical technique, spinal surgery standard of care, or non-pain-management aspects of the patient's care are outside this scope. The retaining attorney should identify the specific standard of care issues to be addressed at engagement initiation.
Expert Witness Review Process
Medial branch block cases require review of a defined set of records to support a complete medical-legal opinion. The specific records relevant to the engagement depend on the scope — causation, medical necessity, standard of care, or future care — and are defined in consultation with retaining counsel. Typical records include:
- › Complete treating pain management records — Initial evaluation, follow-up clinical notes, pre-procedure assessments, and post-procedure response documentation for each encounter
- › Procedure reports and fluoroscopy documentation — Imaging records of needle placement, contrast injection, and the procedural record for each block performed, including levels treated and agents used
- › Pre-procedure spinal imaging — MRI or CT of the relevant spinal segment to evaluate degenerative findings, disc pathology, nerve compression, and structural changes at the proposed treatment levels
- › Post-procedure pain assessment records — Documentation of the percentage and duration of pain relief following each block, which constitutes the diagnostic foundation for the MBB result and the basis for any subsequent procedure authorization
- › Billing records — Itemized billing by CPT code and date of service, to evaluate consistency between procedures billed and procedures documented in the clinical record
- › Insurance correspondence and authorization records — Pre-authorization requests, payer criteria applied, and denial or approval documentation, where a necessity dispute is at issue
- › Prior treating physician records — Records predating the pain management relationship, to establish baseline symptom status, pre-existing history, and prior treatment course
- › Deposition testimony — Testimony of the treating pain management physician, the claimant, and any other retained experts, addressing the clinical rationale, patient-reported response, and contested factual issues
Contact Expert Medical Services LLC with a brief case summary and a description of the available records. Engagements may address medical necessity, standard of care, causation, or future medical care projections and can be structured to address one or more of these issues within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Radiofrequency Ablation
Expert review of RFA medical necessity, standard of care, and the diagnostic pathway from medial branch blocks.
Epidural Steroid Injections
Expert evaluation of ESI medical necessity, causation, and standard of care in personal injury and malpractice matters.
CRPS Expert Witness
Complex Regional Pain Syndrome — diagnosis, causation, and future care review.
Spinal Cord Stimulation
Medical necessity, cost projections, and expert testimony on neuromodulation.
Post-Laminectomy Syndrome
Persistent spinal pain after surgery — causation, standard of care, and future care review.
Future Medical Care Review
Projecting ongoing pain management costs for damages analysis.
Causation Analysis
Establishing whether the subject incident produced or aggravated facet-mediated spinal pain.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for medial branch blocks — diagnostic adequacy and RFA predicate sequencing.
Standard of Care Analysis
Standard of care analysis for diagnostic medial branch block protocols and RFA candidacy determination.
FAQ
Medial Branch Block — Common Attorney Questions
- A medial branch block is a fluoroscopically guided injection of local anesthetic onto the medial branch nerves that carry sensory signals from the cervical or lumbar facet joints. When performed diagnostically, the procedure evaluates whether the facet joint is a clinically significant pain generator. When performed therapeutically, it provides temporary relief of axial spinal pain. Medial branch blocks are a standard interventional pain management procedure and a prerequisite diagnostic step before radiofrequency ablation in most clinical settings.
- Medical necessity for a medial branch block is typically supported by documented axial spine pain consistent with facet-mediated origin, physical examination findings compatible with the proposed diagnosis, relevant imaging, and a clinical course that has not resolved with conservative management. The procedure is generally indicated when the facet joint is a plausible pain generator and the diagnostic information will guide further treatment decisions. Necessity is evaluated on a case-specific basis against the clinical record and applicable treatment guidelines.
- Most clinical guidelines and payer policies require documentation of two separate confirmatory medial branch blocks — each producing a defined percentage of pain relief (typically 50% to 80% improvement) for a duration consistent with the anesthetic agent used — before radiofrequency ablation is authorized. The percentage improvement and duration of relief should be documented contemporaneously in the procedure record. Absence of this documentation is one of the most common medical necessity and standard of care issues in medial branch block and RFA litigation.
- The causal question is whether the accident produced or aggravated facet-mediated cervical or lumbar pain sufficient to require interventional treatment. Rear-impact motor vehicle collisions can produce cervical facet joint injuries through hyperextension-flexion mechanisms. Lumbar facet injuries may occur from axial loading or rotational forces. Causation review addresses the temporal relationship between the accident and symptom onset, the mechanism of injury, pre-existing degenerative findings, and the clinical documentation from the relevant period.
- Medial branch blocks are generally considered low-risk procedures when performed under fluoroscopic guidance with appropriate technique. Recognized complications include intravascular injection of local anesthetic, infection at the injection site, hematoma, vasovagal response, allergic reaction, inadvertent epidural or subarachnoid spread, and nerve injury from direct needle trauma. The incidence of serious complications is low, but failure to use fluoroscopic guidance, improper needle placement, or inadequate patient monitoring may elevate procedural risk and is relevant to standard of care review.
- Malpractice review addresses whether the care provided met the applicable standard of care for a board-certified pain management physician performing medial branch blocks. The evaluation considers patient selection, pre-procedure documentation, use of fluoroscopic guidance, informed consent, post-procedure monitoring, and the clinical rationale for the number of procedures performed. Where complications occurred, review addresses whether they resulted from a deviation from the standard of care or from a recognized risk of the procedure.
- Key records include the complete treating pain management notes, procedure reports and fluoroscopy documentation, pre-procedure imaging (MRI or CT of the relevant spinal segment), post-procedure pain assessment records documenting percentage relief and duration, billing records, insurance correspondence and authorization records, prior treating physician records predating the pain management relationship, and, where applicable, deposition testimony of the treating pain management physician.
- A positive diagnostic response is generally defined as at least 50% reduction in targeted axial pain lasting for the expected duration of the local anesthetic used. Some guidelines require 80% relief. A positive response on two confirmatory blocks — ideally using different local anesthetic agents to control for placebo response, with the duration of relief correlating to the agent used — is the standard basis for proceeding to radiofrequency ablation. Inconsistent documentation of relief percentage and duration is a frequent point of dispute in both medical necessity and standard of care review.
Retain a Medial Branch Block Expert for Your Case
Dr. Dardashti accepts medial branch block and radiofrequency ablation engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.