Nationwide Pain & Injury Medical Expert Witness
Medical Necessity Review — Pain Management
Physician-level medical necessity analysis for pain management procedures, implanted devices, interventional treatments, and future care projections. Written opinion structured for deposition and trial. Plaintiff and defense.
Request AvailabilityCredentials & Qualifications
- Service
- Medical Necessity Review & Written Opinion
- Specialty
- Pain Management & Anesthesiology
- Standards Applied
- Clinical Guidelines, Peer-Reviewed Evidence
- Report Format
- Written Opinion, Supplemental Available
- Available For
- Plaintiff & Defense
- Jurisdiction
- California — Nationwide
What Is Medical Necessity?
Medical necessity is a clinical determination — not a billing term, not a payer category, and not synonymous with a treating physician's recommendation. A treatment is medically necessary when the documented diagnosis, the patient's clinical presentation, and the published evidence base together support that specific intervention at that point in the patient's care trajectory. A physician's recommendation that a treatment would benefit the patient does not, by itself, establish that it was medically necessary under the applicable clinical standard.
The distinction between a treatment recommendation and a medical necessity determination is one of the most persistently misunderstood concepts in pain management litigation. Treating physicians recommend treatment based on their clinical judgment, their therapeutic relationship with the patient, and their assessment of probable benefit. Medical necessity is evaluated after the fact — against the published indications, prerequisite requirements, and documentation criteria that govern the specific procedure. A physician can reasonably recommend a treatment that does not satisfy the formal necessity criteria. Conversely, a treatment that a payer or defense expert calls unnecessary may be well-supported by the specialty literature the treating physician applied.
Medical necessity disputes arise in pain management litigation primarily because chronic pain treatment involves escalating interventions — each step of which has documented indications, failure-of-conservative-care prerequisites, and published guidelines — and because the financial stakes of expensive interventional procedures and implanted devices are high enough to make each step worth contesting. The articles on how pain management experts evaluate medical necessity in personal injury cases and on the difference between medical necessity and standard of care address these foundational issues in greater depth.
Why Medical Necessity Matters in Litigation
Medical necessity is a threshold question in virtually every pain management damages dispute. It determines whether treatment was compensable, whether future care projections are supportable, whether insurance coverage applies, and whether a treating physician's decisions are defensible against a malpractice claim. Despite its centrality, medical necessity is frequently litigated on inadequate evidence — payer denial letters and unsupported assertions from treating physicians who have never articulated the clinical basis for the treatment they rendered.
When a medical necessity dispute reaches a jury, the question is not whether a payer's criteria were met but whether the treatment was clinically appropriate for the patient's documented condition under the standards that govern physician practice. That question requires a physician expert with a complete medical record review, not a claims adjuster or non-treating reviewer who evaluated a summary.
In personal injury and malpractice litigation, medical necessity disputes commonly arise in three distinct contexts:
- Coverage disputes: Whether an insurer's denial of treatment authorization was supported by the clinical record and applicable guidelines, or whether the denial was pretextual, non-individualized, or inconsistent with the evidence.
- Damages disputes: Whether treatment already rendered was medically necessary and therefore compensable as a litigation damage, or whether the treatment was elective, premature, or beyond what the diagnosis supported.
- Future care disputes: Whether proposed future treatment — including implanted devices, repeat injections, long-term medication management, or surgical intervention — is medically indicated for the documented condition, and whether the proposed cost projection reflects that indication.
In each context, the medical necessity opinion is the evidentiary centerpiece of the dispute. An opinion that cannot withstand cross-examination on the clinical standards applied, the record reviewed, and the reasoning employed will not sustain a damages award or prevail on a coverage motion.
How Pain Management Experts Evaluate Medical Necessity
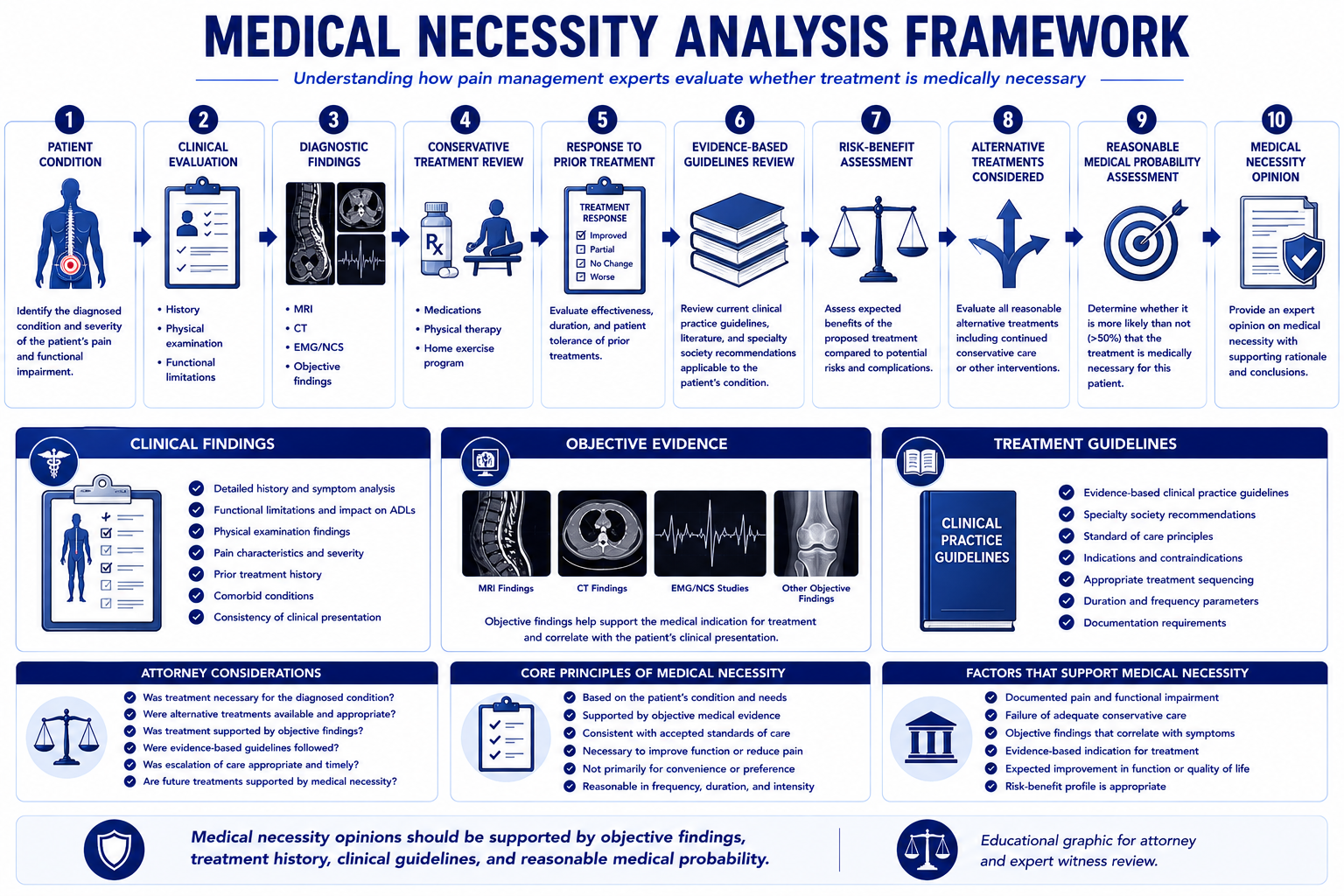
A defensible medical necessity opinion is not a summary conclusion. It is a structured analytical process that moves from documented clinical findings to the applicable guideline standard to a reasoned conclusion. The following elements constitute the analytical framework a qualified pain management expert applies.
History and Clinical Presentation
Medical necessity analysis begins with the patient's documented history — the onset of symptoms, the mechanism of injury, the character and distribution of pain, and the prior treatment course. The history establishes whether the condition is consistent with the diagnosis claimed and whether the treatment trajectory reflects an appropriate escalation of care. A history that shows no documentation of the symptom pattern required to support the proposed treatment — for example, no documented radicular symptoms in a claim for transforaminal epidural steroid injections — is a fundamental gap in the necessity foundation.
Physical Examination Findings
Physical examination findings are the objective clinical anchor of the medical necessity determination. For interventional pain procedures, published guidelines typically specify examination criteria — positive provocative tests, neurological deficits consistent with the claimed radicular distribution, range-of-motion limitations corroborating the structural diagnosis, or specific sensory and motor findings consistent with the nerve at issue. Examination findings documented in the treating record that are inconsistent with the claimed diagnosis, or that are entirely absent despite a diagnosis that requires positive physical findings, weaken the medical necessity foundation for treatment directed at that diagnosis. For the complete methodology a pain management physician uses to conduct an objective evaluation — examination, imaging correlation, validated instruments, and functional capacity — see the article on how pain management experts objectively evaluate pain.
Imaging Correlation
Imaging must correlate with both the clinical diagnosis and the treatment approach. The medical necessity analysis examines whether the imaging findings — disc herniation level, stenosis pattern, facet joint changes, nerve root impingement — correspond to the symptomatic level, the side of symptoms, and the specific procedure performed. Treating at a level or side not supported by the imaging and examination is a common source of medical necessity challenges. For interventional procedures, fluoroscopic guidance is required not only for technical accuracy but also as documentation that the procedure was directed at the structurally relevant pathology.
Functional Limitations
Medical necessity for most pain management interventions requires documented functional impairment — not merely subjective pain complaints. Published guidelines for epidural steroid injections, radiofrequency ablation, and neuromodulation typically require that the pain be causing measurable functional limitations affecting activities of daily living, occupational function, or ambulation. A treating record that documents only numerical pain scores without functional correlates provides a weaker medical necessity basis than one that documents specific functional deficits the proposed treatment is expected to address. The same objective functional documentation that supports medical necessity also underpins non-economic damages claims; for the rational evidentiary connection standard governing objective evidence and pain and suffering in Texas, see the Gregory v. Chohan pain and suffering damages guide.
Prior Treatment Response
The single most frequently litigated medical necessity element is the failure-of-conservative-care prerequisite. For interventional procedures, neuromodulation, and surgical intervention, published guidelines uniformly require that a specified course of conservative treatment — physical therapy, non-opioid pharmacological management, activity modification — have been trialed and documented before escalating to the disputed intervention. The medical necessity analysis examines not only whether conservative care was rendered, but whether it was documented with sufficient specificity to satisfy the guideline criteria: duration, modalities, patient response, and the basis for concluding that further conservative management was unlikely to produce meaningful benefit.
Risk-Benefit Analysis
Medical necessity requires not only that the treatment be indicated but that the expected clinical benefit outweighs the procedural risk for the specific patient. The risk-benefit analysis is particularly important for high-risk patients — those with significant comorbidities, prior surgical complications, coagulopathy, or conditions that increase procedural risk — and for high-risk procedures such as intrathecal pump implantation, spinal cord stimulator revision, or repeat epidural procedures in the setting of prior complications. The absence of a documented risk-benefit discussion in the treating record is a medical necessity gap that the expert opinion must address.
Evidence-Based Medicine
The published evidence base for each procedure establishes the clinical necessity threshold: what level of pain, what diagnostic criteria, what failure of prior treatment, and what expected benefit the literature supports. The medical necessity opinion must engage this literature directly — not by citing guidelines as a checklist, but by identifying the specific evidentiary standard that applies to the procedure and explaining how the documented clinical facts do or do not satisfy it. An expert who cannot identify the relevant guidelines, cannot articulate what they require, and cannot explain how the documented care compares to those requirements will not withstand cross-examination.
Procedure-Specific Medical Necessity Analysis
Each pain management procedure has distinct indication criteria, prerequisite documentation requirements, and characteristic litigation dispute patterns. The following analysis addresses the procedures most commonly at issue.
Epidural Steroid Injections
Epidural steroid injections (ESIs) are among the most common pain management procedures and among the most frequently challenged on medical necessity grounds.
Typical indications: Radicular pain or neurogenic claudication caused by disc herniation, spinal stenosis, or foraminal narrowing at an identified level, with corresponding neurological symptoms and imaging correlation. The injection approach — interlaminar, transforaminal, or caudal — must be appropriate for the documented pathology and symptomatic level.
Documentation requirements: Documented radicular symptoms with dermatomal distribution; imaging identifying the structural correlate; failure or inadequacy of conservative pain management; fluoroscopic guidance to confirm needle placement; and documented response to each injection in the series before repeating.
Common deficiencies: Absence of documented conservative care preceding the injection series; injections performed at levels not supported by the imaging; fluoroscopic guidance not used without documented rationale; no documented response assessment before repeat injection; frequency exceeding published guideline limits without clinical justification.
Litigation disputes: Carrier denial for lack of imaging correlation; defense challenge to frequency of serial injection series; disputes about whether documented conservative care was adequate before injection; future care projections of indefinite injection series without clinical rationale.
Medial Branch Blocks and Radiofrequency Ablation
Medial branch blocks (MBBs) are diagnostic procedures used to confirm facet-mediated pain before proceeding to radiofrequency ablation (RFA).
Typical indications: Axial spinal pain — cervical, thoracic, or lumbar — with a clinical presentation consistent with facet-mediated origin: non-radicular distribution, reproduction of pain with facet loading maneuvers, absence of neurological deficit. Imaging may show facet joint changes but imaging alone does not establish facet-mediated pain.
Documentation requirements: Two diagnostic MBBs at each level before proceeding to RFA, with documented percentage of pain relief meeting the published threshold (typically 50% or 80% depending on the guideline applied); documented duration of relief; technique confirmation of needle placement at the medial branch; RFA technique appropriate for the level treated.
Common deficiencies: Only one diagnostic block performed before RFA; percentage of pain relief not documented or below threshold; MBB response assessed at an interval inconsistent with the anesthetic used; repeat RFA performed without documentation of prior response duration; levels treated on RFA do not match levels blocked diagnostically.
Litigation disputes: Carrier denial for inadequate diagnostic block documentation; defense challenge to whether the MBB response met the threshold for RFA; disputes about repeat RFA intervals and whether prior response justified retreatment; future care projections of annual or biennial RFA without prior documented response pattern.
Spinal Cord Stimulation
Spinal cord stimulation (SCS) is one of the most contested medical necessity determinations in pain management litigation because of its high cost and the complexity of its indications. For a detailed discussion of SCS medical necessity in litigation, see the article on how pain management experts evaluate medical necessity for spinal cord stimulators.
Typical indications: Post-laminectomy syndrome, CRPS, refractory radiculopathy, peripheral neuropathy, and other chronic neuropathic pain conditions that have not responded to conservative and interventional management. The diagnosis must be documented and consistent with published SCS indications; SCS is not indicated for nociceptive pain or for conditions with surgically correctable pathology not yet addressed.
Documentation requirements: Documented failure of a meaningful trial of conservative care, pharmacological management, and appropriate interventional procedures; psychological evaluation and psychosocial screening completed before implant; trial stimulation period (typically 3–7 days) with documented pain relief ≥50% and functional improvement; technical documentation of trial lead placement, stimulation parameters, and patient-reported response.
Common deficiencies: Conservative care not documented before escalating to neuromodulation; psychological screening absent or inadequate; trial response not documented with percentage of pain relief; permanent implant placed after an inadequate trial period; patient reported subjective improvement without objective functional documentation.
Litigation disputes: Defense challenge to whether failure-of-conservative-care was documented for the specific SCS indication; challenge to adequacy of the trial response; claims that the patient's comorbidities or diagnosis does not fall within published SCS indications; future care projections of SCS battery replacement intervals — see the spinal cord stimulation expertise page for device-specific discussion.
Intrathecal Pump Therapy
Intrathecal pump therapy (ITP) delivers medication directly into the intrathecal space via an implanted catheter and pump.
Typical indications: Chronic refractory pain conditions — including cancer pain, post-laminectomy syndrome, CRPS, and spasticity — where systemic opioid or pharmacological management has produced inadequate relief or intolerable side effects. PACC guidelines specify patient selection criteria including diagnosis, prior treatment history, psychological screening, and intrathecal drug trial requirements.
Documentation requirements: Systemic opioid or pharmacological therapy documented as inadequate or intolerable; PACC-compliant patient selection criteria satisfied; intrathecal drug trial demonstrating adequate analgesia before permanent implant; psychological evaluation completed; risks and alternatives discussed and documented.
Common deficiencies: Escalation to ITP without documented failure of systemic pharmacological management; intrathecal trial not performed or poorly documented; patient selection criteria not formally assessed against PACC criteria; refill visit records absent, limiting future care projection support.
Litigation disputes: Necessity of escalation to ITP versus alternative pain management strategies; pump replacement interval disputes in future care projections; complications attributed to inadequate patient selection; disputes about whether the documented diagnosis fell within published ITP indications.
Peripheral Nerve Stimulation
Peripheral nerve stimulation (PNS) applies electrical stimulation to a targeted peripheral nerve to modulate neuropathic pain. The published indications for PNS are more limited than for SCS, and the evidentiary support for specific applications is evolving.
Typical indications: Refractory neuropathic pain in the distribution of a specific peripheral nerve — occipital neuralgia, ilioinguinal, genitofemoral, or supra-orbital nerve distributions — where the nerve target has been identified with diagnostic precision and pharmacological and interventional management have been trialed.
Documentation requirements: Identification of the specific peripheral nerve target with supporting diagnostic nerve block or imaging; documented failure of prior conservative and interventional treatment; percutaneous trial demonstrating adequate pain relief; technical documentation of electrode placement and trial response.
Common deficiencies: Nerve target not confirmed with diagnostic precision before implant; trial period inadequately documented; application to an indication with limited evidentiary support in the published literature at the time of implantation.
Litigation disputes: Carrier denial for indications not explicitly covered by coverage policies; defense challenge to whether the evidentiary basis for the specific PNS application met the clinical necessity threshold; future care projections for devices with shorter published longevity data.
Medical Necessity vs. Standard of Care
Medical necessity and standard of care are related but analytically distinct concepts. Attorneys who conflate them invite problems at deposition and trial that a prepared opposing expert will exploit. For a detailed analysis of this distinction, see the article on what is the difference between medical necessity and standard of care.
Medical necessity is a threshold determination: was the treatment clinically indicated for this patient's documented condition? It asks whether intervention was warranted at all — whether the diagnosis justified the proposed treatment, whether conservative measures were appropriately trialed first, and whether the selected modality was within the published indications for that diagnosis.
Standard of care is a performance determination: if the treatment was indicated, was it performed in conformity with accepted clinical practice? It asks whether the physician who performed the procedure did so in a manner consistent with what a qualified specialist would do under similar circumstances — addressing technique, documentation, informed consent, complication management, and follow-up.
A procedure can be medically necessary but performed below the standard of care. A procedure can also be performed flawlessly but not medically indicated in the first place. Both issues arise in pain management malpractice, personal injury, and insurance coverage litigation. When both are in dispute, each requires a separate analytical framework in the expert opinion, and each will be addressed separately on cross-examination.
Consider the most common scenario where the distinction becomes consequential: a patient undergoes a lumbar radiofrequency ablation that is technically performed correctly — but the diagnostic medial branch block sequence was incomplete, and the percentage of pain relief documented was below the guideline threshold for proceeding to RFA. The standard of care for the ablation technique may have been met; the medical necessity of proceeding to ablation at all was not. A standard-of-care opinion that addresses only the technique will not reach the necessity question, and vice versa. For cases requiring both analyses, see the standard of care analysis service page.
Medical Necessity and Causation
In personal injury litigation, causation and medical necessity are the two most frequently contested physician-opinion issues — and they are not the same question.
Causation asks: did the subject incident produce the condition that required treatment? The causal analysis evaluates the mechanism of injury, the temporal onset of symptoms, the pre-incident medical baseline, and the biological plausibility of the claimed causal pathway.
Medical necessity asks: given the documented condition — however it arose — was the treatment rendered or proposed clinically warranted? The medical necessity analysis evaluates whether the diagnosis justified the treatment, not how the diagnosis came about.
Both issues arise in most personal injury cases, and both must be addressed with physician-level specificity. A defense expert who concedes causation but challenges medical necessity forces the plaintiff to defend each treatment decision on its clinical merits. A plaintiff expert who establishes causation but cannot defend the necessity of expensive interventional or device-based treatment is vulnerable on the damages side.
Several causation-adjacent questions directly affect the medical necessity analysis:
- Aggravation of pre-existing conditions: When the incident aggravates a pre-existing degenerative condition, the medical necessity analysis must distinguish between treatment directed at the new aggravation and treatment for the underlying pre-existing pathology that would have been required regardless of the incident. This line is often the most consequential factual dispute in the case.
- Pre-existing degeneration: Multi-level degenerative disc disease or facet arthrosis that predates the incident does not automatically render treatment for the incident-related aggravation medically unnecessary — but it does require the expert to explain which clinical findings reflect new pathology rather than the natural history of pre-existing disease.
- Subsequent injuries: When the claimant sustains a subsequent injury after the subject incident, the medical necessity analysis must apportion treatment between the two events. Treatment that would have been necessary regardless of the subsequent injury remains causally attributable to the first incident; treatment rendered necessary by the subsequent injury may not be.
- Future treatment necessity: The necessity of projected future care depends on the same causation framework — projected treatment for the incident-related condition is compensable; projected treatment for conditions not causally attributable to the incident is not. The necessity and causation analyses must be consistent in the expert's opinion.
For cases requiring both opinions, see the causation analysis service page. Dr. Dardashti can provide both analyses in a single engagement or in sequenced opinions depending on the case timeline.
Common Medical Necessity Disputes
The following categories represent the most frequently litigated medical necessity disputes in pain management matters. Understanding each dispute type — and the clinical arguments on both sides — allows attorneys to evaluate their evidentiary position before retaining an expert.
- Excessive injections: A series of epidural steroid injections, nerve blocks, or facet injections that exceeds published frequency limits without documented clinical justification. Published guidelines typically limit epidural steroids to three to four injections per spinal region per year; more frequent injections require documented failure of prior injections and clinical justification. Defense experts challenge both the necessity of the first series and the decision to repeat without documented benefit. Plaintiff experts counter with documented improvement in function or pain between injection cycles.
- Repeated procedures with little documented benefit: A pattern of repeated interventional procedures in which the treating record does not document the patient's response to each procedure before repeating it. Without response documentation, the clinical justification for repetition is absent, and the medical necessity of the series is vulnerable. This issue arises frequently in cases involving multiple epidural series or serial medial branch blocks where no systematic response assessment was recorded between procedures.
- Premature spinal cord stimulation: SCS performed before a documented adequate trial of conservative care and less invasive interventional management for the specific SCS indication. The defense position is that the treating physician escalated to neuromodulation without exhausting the prerequisite treatment steps. The plaintiff position is that prior treatment was adequate and documented. The expert's analysis examines the specific prior treatment documented — modalities, duration, patient response — against the published SCS candidacy criteria for the diagnosed condition.
- Unsupported future care projections: A life care plan or future care projection that includes treatments, frequencies, or devices not grounded in the clinical record or published guidelines for the documented diagnosis. Common examples include: projection of indefinite injection series without prior documented benefit pattern; SCS battery replacement intervals shorter than manufacturer data supports; future opioid management projected at doses above CDC guideline thresholds without clinical rationale. Each projected line item must withstand independent necessity scrutiny.
- Revision surgeries and device replacements: Revision of an implanted spinal cord stimulator, intrathecal pump exchange, or peripheral nerve stimulator requires the same medical necessity foundation as the original implant — the documented clinical indication for the revision must be addressed. Routine device replacement at the end of battery life is generally supported by published device longevity data; revision for inadequate pain control, lead migration, or device failure requires additional clinical documentation establishing that the device continues to be medically necessary and that the revision is expected to restore clinical benefit.
- Long-term opioid therapy: Medical necessity of long-term opioid management is evaluated against CDC prescribing guidance, state medical board guidelines, and the specific clinical picture — the diagnosis, the treatment alternatives trialed, the patient's documented functional status, and the risk-benefit profile at each prescribing decision. Disputes arise about whether opioids were necessary for the documented condition, whether doses were within published guidelines, whether appropriate functional monitoring was documented, and whether non-opioid alternatives were adequately trialed. In personal injury cases with lien-based treatment, opioid prescribing patterns are also evaluated for consistency with independent clinical decision-making.
Plaintiff and Defense Perspectives
Plaintiff Arguments
Plaintiff experts in medical necessity disputes establish that the treating record contains adequate documentation of the clinical prerequisites for the disputed treatment. The central arguments are: that the diagnosis is supported by examination and imaging; that conservative care was trialed and documented before escalation; that published guidelines support the specific modality and frequency of treatment rendered; that any payer denial was based on administrative criteria more restrictive than the applicable clinical standard; and that the treating physician's clinical judgment was exercised in a manner consistent with what a qualified specialist would do in the same circumstances.
For CRPS cases specifically, plaintiff experts must address the Budapest Criteria documentation — ensuring that the diagnosis is supported by documented examination findings at each clinical encounter, not only by symptom reports. A CRPS diagnosis that rests on subjective symptom reports without the required objective examination signs is a structural weakness that defense experts will exploit. See the CRPS expert witness guide for the full diagnostic and medical necessity framework in CRPS litigation.
Defense Arguments
Defense experts target the weakest documentation links in the treating record. The most effective defense arguments in medical necessity disputes are not broad attacks on the treatment philosophy — they are specific, record-grounded arguments that a specific prerequisite was not documented, a specific guideline criterion was not met, or a specific clinical finding required by the published indication was absent.
The most frequently advanced defense positions: conservative care was not adequately documented before escalating to interventional or device-based treatment; the diagnosis is not supported by objective findings consistent with the published indication criteria; the frequency of procedures exceeded guideline limits; the diagnostic block response for RFA was below threshold; the SCS trial response was inadequately documented; and the future care projection exceeds what the clinical record supports. Each position is most effective when it is anchored in a specific guideline provision — not a generalized assertion that the treatment was unnecessary.
Rebuttal Analysis
When an opposing medical necessity opinion has already been produced, a targeted rebuttal addresses each specific clinical argument advanced — not by reciting the treating record but by engaging the specific standard the opposing expert applied and explaining where that application is inconsistent with the full record, the applicable guideline version in effect at the time of treatment, or the clinical evidence base. Effective rebuttal identifies the specific passages in the opposing report that are inconsistent with the record, the specific guideline provisions that contradict the opposing expert's characterization, and any clinical evidence the opposing expert did not address or mischaracterized.
Rebuttal opinions are available as supplemental declarations, written reports, or deposition testimony prepared after review of the opposing expert's report. For cases also requiring an independent medical evaluation, the IME and rebuttal can be structured as a coordinated engagement.
Medical Necessity and Future Medical Care
Every legitimate future medical care projection must be grounded in a medical necessity determination. A proposed future treatment that cannot survive a medical necessity challenge should not appear in a future care projection — and if it does, opposing experts will dismantle it at deposition.
The relationship is this: the future medical care review projects the treatment a claimant will require and its associated costs. The medical necessity review provides the clinical foundation for that projection — the documented diagnosis, the applicable indication, the guideline-based frequency and duration, and the evidence that the proposed modality is appropriate for this patient. Without that foundation, a future care projection is speculative. With it, the projection is defensible at trial.
When future care includes high-cost interventions such as spinal cord stimulation or intrathecal pump therapy, the medical necessity analysis is particularly critical. These devices involve significant implantation costs, follow-up requirements, and device replacement cycles that will be scrutinized by defense experts, insurance carriers, and courts. A future care projection that projects SCS without addressing the medical necessity of neuromodulation for the specific documented condition will not withstand that scrutiny.
Clinical Guidelines and Evidence-Based Review
Medical necessity determinations in pain management are not made in a clinical vacuum. Published guidelines from specialty societies provide the evidentiary framework against which individual clinical decisions are evaluated. Understanding which guidelines apply — and which are most current and authoritative — is essential to an opinion that will withstand cross-examination.
The primary guidelines applied in pain management medical necessity review include:
- ASIPP Evidence-Based Guidelines: The American Society of Interventional Pain Physicians publishes comprehensive evidence reviews covering epidural steroid injections, facet joint interventions, radiofrequency procedures, neuromodulation, and related modalities.
- PACC Consensus Guidelines: The Polyanalgesic Consensus Conference guidelines govern intrathecal drug delivery patient selection, drug protocols, and implantation criteria.
- North American Neuromodulation Society (NANS) Guidelines: Govern patient selection and clinical practice for SCS and PNS.
- CDC Prescribing Guidance: The CDC's clinical practice guideline for prescribing opioids for chronic pain establishes the evidentiary basis for opioid medical necessity assessments in non-cancer chronic pain.
- Payer LCD/NCD Policies: Medicare Local and National Coverage Determinations define coverage criteria that are often adopted as proxy medical necessity standards by commercial payers. Where a payer's internal criteria differ from published guidelines, the discrepancy is itself relevant to the dispute.
Medical Necessity in Personal Injury Cases
In personal injury litigation, medical necessity is a damages question. The defendant argues that treatment was not caused by the accident (causation) or that it was not clinically warranted even if causation is conceded (medical necessity). Both lines of attack target the same goal: reducing or eliminating the compensable damages.
- Diagnostic imaging: Whether the frequency and type of imaging obtained — multiple MRIs, CT myelograms, functional imaging — were clinically indicated given the evolving presentation.
- Interventional procedures: Whether a series of injections, nerve blocks, or ablation procedures was medically warranted, or whether the procedures exceeded the clinical indication for the documented injury.
- Surgical and device-based care: Whether implanted devices, surgical intervention, or spinal procedures were medically necessary at the time they were performed, and whether the escalation from conservative care to invasive treatment was appropriately documented and clinically supported.
- Future care projections: Whether the future treatment proposed by plaintiff's experts is within published guidelines for the documented condition, and whether the proposed cost projection reflects the medically indicated scope rather than the maximum possible treatment.
For California-specific discussion of how medical necessity expert opinions function within the Evidence Code admissibility framework, MICRA damages caps, and the lien-based treatment dynamics that affect necessity documentation in personal injury cases, see the California pain management expert witness guide.
Medical Necessity in Medical Malpractice Cases
In medical malpractice litigation, medical necessity intersects with standard of care in a specific way: the plaintiff must establish not only that the physician's conduct fell below the standard of care, but often that the departure caused identifiable harm — including unnecessary treatment, avoidable complications, or failure to provide care that was warranted.
- Unnecessary procedures: Whether injections, ablation procedures, or implanted devices were performed without adequate clinical indication, exposing the patient to procedural risk without expected therapeutic benefit.
- Inadequate prior authorization documentation: Whether the treating physician failed to document the clinical rationale for treatment in a manner that supports a medical necessity finding.
- Failure to escalate: Whether a treating physician failed to pursue medically necessary treatment — neuromodulation, referral to a specialist, or a specific interventional approach — when the clinical record supported escalation.
- Overprescribing and underprescribing: Whether opioid prescribing exceeded or fell below the medically necessary level for the documented condition, under the applicable prescribing guidelines in effect at the time of the prescribing decision.
Documentation Requirements for Medical Necessity Review
A defensible medical necessity opinion is only as strong as the documentation on which it is based. The following records are required for a complete medical necessity review:
- Treating physician notes: Office visit records from the treating pain physician covering the relevant treatment period, including clinical assessments, diagnosis documentation, and treatment rationale.
- Procedure records: Operative reports, fluoroscopy records, anesthesia records, and post-procedure notes for each intervention at issue.
- Diagnostic imaging reports: MRI, CT, X-ray, and other imaging studies with reports. Imaging findings must correspond to the documented diagnosis.
- Prior treatment records: Documentation of conservative treatment — physical therapy, chiropractic, medication trials — preceding any interventional or device-based care.
- Prior authorization correspondence: Payer authorization requests, denial letters, peer-to-peer review notes, and appeal correspondence.
- Pharmacy records: Medication history relevant to whether pharmacological options were trialed before escalating to procedural intervention.
- Device records: For implanted device disputes — trial records, implant operative reports, device representative records, and post-implant programming notes.
- Psychological evaluation records: Required before implanted device procedures; relevant to the adequacy of the pre-implant evaluation.
- Opposing expert reports: For rebuttal engagements, the opposing expert's written report and any deposition testimony.
How to Request a Medical Necessity Review
Contact Expert Medical Services LLC with the case records, the procedure or treatment at issue, and the specific medical necessity questions to be addressed. Cases involving implanted devices — SCS, ITP, PNS — benefit from early record assembly that includes the full pre-implant evaluation, trial period documentation, and any payer correspondence. For cases also requiring causation analysis, see the causation analysis service. For cases requiring an in-person examination in addition to records review, a concurrent independent medical evaluation may be appropriate. For cases where standard of care is also in dispute, see the standard of care analysis service.
Medical necessity opinions are available as written record review reports, supplemental declarations responding to opposing expert opinions, and deposition or trial testimony. Dr. Dardashti provides opinions for plaintiff and defense counsel, insurance carriers, mediators, and courts in California and nationwide.
Related Services & Expertise
Future Medical Care Review
Evidence-based future care projections grounded in medical necessity analysis for each projected treatment item.
Causation Analysis
Establishing the causal link between injury and diagnosis before evaluating the necessity of treatment.
Independent Medical Evaluation
Structured examination and written opinion addressing diagnosis, causation, medical necessity, and future care.
Standard of Care Analysis
Evaluating whether treatment was performed in conformity with accepted clinical practice — analytically distinct from necessity.
Spinal Cord Stimulation
Medical necessity, candidacy criteria, and device appropriateness for SCS in litigation.
Intrathecal Pump Therapy
Medical necessity review for implanted drug delivery systems, device complications, and future care.
FAQ
Medical Necessity Review — Common Attorney Questions
- A medical necessity review is a physician's structured analysis of whether a specific treatment, procedure, device, or course of care was clinically indicated for the documented diagnosis at the time it was ordered or rendered. In litigation, medical necessity is frequently contested — insurance carriers deny claims based on medical necessity grounds, defendants argue that disputed treatment was unnecessary, and plaintiffs counter that medically appropriate care was improperly withheld or denied. A pain management physician is the appropriate expert to evaluate medical necessity for interventional procedures, implanted devices, long-term opioid management, and other modalities within the specialty.
- Medical necessity determinations in pain management are evaluated against multiple overlapping standards: published clinical guidelines from bodies such as the American Society of Interventional Pain Physicians (ASIPP), the American Society of Anesthesiologists (ASA), and the American Academy of Pain Medicine (AAPM); peer-reviewed medical literature on the efficacy and indications for specific procedures; payer-specific coverage policies where applicable; and the clinical judgment of a qualified pain management specialist applying those standards to the individual patient's documented condition. No single source controls — the physician expert synthesizes all relevant sources and applies them to the specific facts of the case.
- Medical necessity and standard of care are analytically distinct. A medical necessity opinion asks whether a specific treatment was clinically indicated for this patient's documented condition — the threshold question of whether intervention was warranted at all. A standard of care opinion asks whether the treating physician performed that treatment in conformity with accepted clinical practice — the question of how the treatment was performed. Both questions arise in the same cases, but they address different elements. A procedure can be medically necessary but performed below the standard of care, or performed flawlessly but not indicated in the first place. Attorneys handling medical malpractice, insurance coverage, and personal injury disputes frequently need opinions on both, and Dr. Dardashti can address each analytically.
- Causation and medical necessity are related but separate determinations. Causation addresses whether the subject incident produced the condition that required treatment. Medical necessity addresses whether the treatment rendered or proposed is clinically warranted for that condition, regardless of how the condition arose. In practice, both issues arise in most personal injury cases: the defense may challenge both the causal link between the accident and the diagnosis, and the medical necessity of the treatment prescribed for that diagnosis. Attorneys should understand that each requires an independent analysis, though a single expert can address both in the same opinion.
- Yes. Implanted neuromodulation devices — including spinal cord stimulators and intrathecal drug delivery systems — are among the most frequently contested medical necessity issues in pain management litigation because of their high cost and the specificity of their indications. A medical necessity review for an implanted device addresses: whether the underlying diagnosis is supported; whether conservative and interventional treatments were trialed and documented before escalating to neuromodulation; whether the diagnostic trial period was adequate; whether the patient was an appropriate candidate based on published selection criteria; and whether prior authorization or insurance denial decisions were clinically well-founded or unsupported. Dr. Dardashti evaluates these questions from both plaintiff and defense perspectives.
- A complete medical necessity review requires the full set of treating records covering the relevant period — physician notes, procedure records, diagnostic imaging reports, pharmacy records, prior authorization correspondence, denial letters, and appeal responses. For device-based disputes, operative reports, trial stimulation records, and device representative notes are also relevant. The more complete the record, the more specific and defensible the opinion. Incomplete records can limit the scope of the opinion, and gaps in documentation are themselves a relevant finding when evaluating whether medical necessity was properly established by the treating physician.
- Yes. Dr. Dardashti provides medical necessity opinions for plaintiff and defense counsel. Plaintiff attorneys retain him to establish that treatment that was denied by a payer or contested by the defense was clinically indicated and within the standard of care. Defense attorneys retain him to evaluate whether claimed treatment was medically justified, whether the proposed future care plan is within guideline parameters, and whether the clinical record supports the scope and duration of treatment being claimed. The opinion follows the evidence regardless of which side retains the expert.
- Medical necessity is the foundation of every legitimate future medical care projection. A future care projection that includes treatments, procedures, or devices not clinically indicated for the documented diagnosis is vulnerable to expert challenge and judicial scrutiny. Dr. Dardashti's future care projections are grounded in a medical necessity analysis for each projected item — linking the proposed treatment to a documented diagnosis, a published clinical indication, and a trajectory of care that supports the projection. In many cases, medical necessity review and future medical care projection are performed together, with the necessity analysis serving as the clinical rationale for each projected cost line.
- Most payer and litigation definitions of medical necessity require that the treatment be consistent with accepted clinical standards and supported by adequate evidence — explicitly excluding experimental or investigational procedures. In pain management, the boundary between established and investigational is not always clear. Ketamine infusion therapy, certain neuromodulation approaches, and emerging regenerative treatments occupy a contested evidentiary space where the designation of 'experimental' may or may not reflect current peer-reviewed evidence. A physician expert can address whether a contested treatment meets the medically accepted standard for necessity or falls into the investigational category under the relevant guidelines and literature.
- Yes. Long-term opioid prescribing is among the most contested medical necessity issues in pain management, arising in personal injury and medical malpractice claims. A medical necessity review of opioid therapy addresses whether the diagnosis justified opioid management, whether non-opioid alternatives were appropriately trialed, whether the dose and duration were within published guideline parameters, whether functional monitoring was documented, and whether prescription practices conformed to California Medical Board guidance and CDC prescribing recommendations. Dr. Dardashti evaluates these questions in matters involving both the prescribing physician and the coverage dispute.
- Yes. Reasonable and medically necessary are not synonymous. A treating physician may exercise reasonable clinical judgment in recommending a treatment that another qualified physician would conclude was not clinically indicated under published guidelines — the reasonableness of the recommendation does not resolve the necessity question. Medical necessity is evaluated against the evidentiary standard for the specific treatment: whether the documented diagnosis met the applicable guideline threshold, whether prerequisite treatments were trialed and documented, and whether the clinical picture supported the specific modality chosen. A treatment that falls within a range of reasonable physician discretion may still be challenged as unnecessary if it does not satisfy the necessity criteria for that procedure.
- Yes. Medical necessity is not a static determination — it applies to a specific treatment at a specific point in the clinical trajectory. A treatment that was not medically necessary six months after an injury may become necessary once conservative care has been exhausted. Conversely, a treatment that was initially necessary may become unnecessary once the patient reaches maximum medical improvement or once the clinical condition has resolved. In litigation, the temporal dimension of necessity is particularly important in disputes about the timing of escalation to interventional or device-based care, and in future care projections that span years or decades.
- When a subject incident aggravates a pre-existing condition, the medical necessity analysis must distinguish between treatment directed at the new aggravation and treatment that addresses the underlying pre-existing pathology. Treatment for the aggravated component is potentially compensable and subject to a necessity determination based on the aggravation; treatment for the pre-existing condition that would have been required regardless of the incident is not. This distinction is frequently contested in cases where the claimant has multi-level degenerative spine disease, a prior injury at the same anatomical region, or a chronic pain condition that existed before the subject incident. The expert must engage the treating record carefully to draw the line between incident-related and pre-existing-condition-related necessity.
Request a Medical Necessity Review
Available for plaintiff and defense. Contact Expert Medical Services LLC with case records, the procedure or treatment at issue, and the specific questions to be addressed.