Nationwide Pain & Injury Medical Expert Witness
Independent Medical Evaluations
Objective medical evaluation and written opinion by a board-certified pain management physician. Available for plaintiff and defense in personal injury and related matters.
Request AvailabilityCredentials & Qualifications
- Service
- Independent Medical Evaluation (IME)
- Specialty
- Pain Management & Anesthesiology
- Board Certification
- American Board of Anesthesiology
- Report Format
- Written Opinion Letter
- Available For
- Plaintiff & Defense
- Jurisdiction
- California — Nationwide
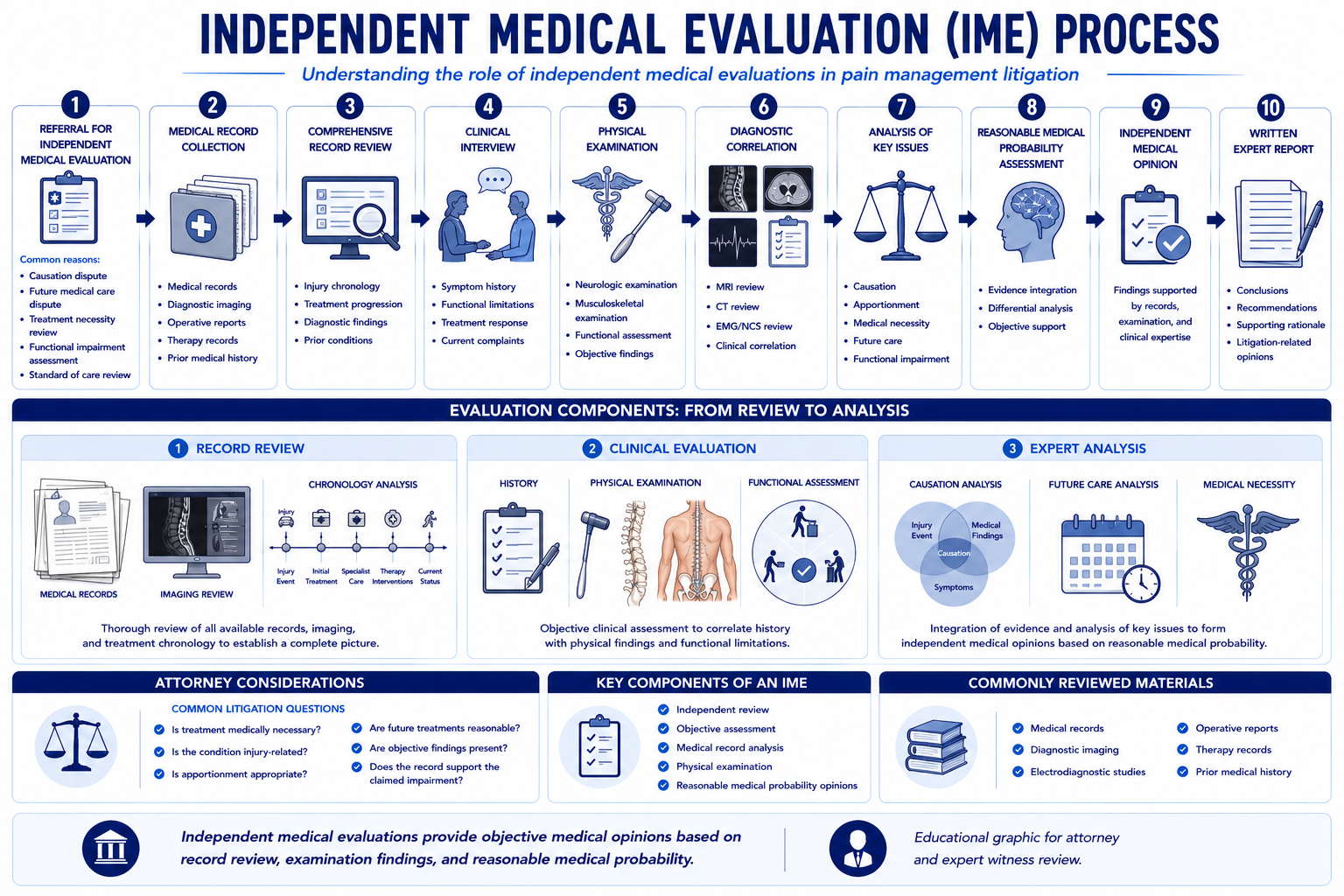
What Is an Independent Medical Evaluation?
An independent medical evaluation (IME) is a structured clinical examination performed by a physician who has no prior treating relationship with the individual being evaluated. The IME physician reviews the available medical records, conducts a physical and clinical examination, and prepares a written report addressing the medicolegal questions specified by the retaining party.
In pain management litigation, IMEs are used to obtain a clinical opinion independent of the treating physician's perspective. The IME report may support or dispute the treating physician's findings — what matters is that it reflects an accurate reading of the medical evidence, not the interests of any party. Pain management IMEs are typically requested in personal injury cases, insurance coverage matters, and malpractice litigation involving interventional procedures or implantable devices.
What Questions Can a Pain Management IME Answer?
The scope of a pain management IME is determined by the specific questions the retaining attorney poses at intake. The following opinion areas are the most frequently requested and represent the full range of clinical questions a board-certified pain management physician is positioned to address.
Diagnosis
The IME physician evaluates whether the claimed diagnosis is supported by the clinical evidence — including examination findings, imaging, electrodiagnostic studies, and the treating record. In pain management cases, diagnostic disputes frequently arise with conditions such as complex regional pain syndrome (CRPS), where the Budapest Criteria must be satisfied by documented examination findings rather than symptom reports alone, and post-laminectomy syndrome, where the clinical picture often overlaps with both surgical sequelae and pre-existing degeneration. The IME physician may confirm the treating diagnosis, modify it based on examination findings, or identify an alternative diagnosis that better accounts for the clinical picture.
Causation
Causation analysis addresses whether the documented diagnosis bears a clinically supported causal relationship to the incident at issue — typically expressed to a reasonable degree of medical probability. The causation opinion reviews the mechanism of injury and its adequacy to produce the claimed condition, the pre-existing medical history and clinical baseline, the temporal relationship between the incident and the onset of documented findings, and the adequacy of competing explanations. For a detailed overview of the causation analysis framework applicable across pain management litigation, see the dedicated service page.
Aggravation of Pre-Existing Conditions
Many chronic pain cases involve claimants with documented pre-existing degenerative spine disease, prior injuries, or prior pain conditions. The IME physician addresses whether the subject incident aggravated, activated, or accelerated a pre-existing condition — and, where possible, distinguishes what portion of the current clinical picture reflects new injury versus pre-existing pathology versus natural disease progression. This clinical apportionment analysis provides the foundation for the jury's legal apportionment determination under the applicable comparative fault or aggravation doctrine framework. For a detailed examination of the clinical methods used to distinguish pre-existing degeneration from traumatic aggravation in spine injury cases, see the article on pre-existing degeneration vs. aggravation in spine injury cases.
Apportionment
In cases with multiple potential contributing causes — a prior injury, a subsequent incident, or concurrent degenerative disease — the IME physician may be asked to address apportionment: what portion of the current condition is attributable to the subject incident versus other contributing factors. Apportionment opinions are clinical, not legal determinations — the physician does not assign legal liability percentages but provides the clinical analysis of causative contribution that the trier of fact uses to perform the legal apportionment.
Medical Necessity
The IME physician evaluates whether treatment rendered — or proposed for the future — was medically necessary based on the clinical record and applicable specialty society guidelines. Necessity disputes in pain management cases most commonly arise with interventional procedures (epidural steroid injections, medial branch blocks, radiofrequency ablation) and with implantable devices (spinal cord stimulation, intrathecal drug delivery systems), where the necessity criteria are specific and the documentation requirements are demanding. The IME necessity opinion identifies the applicable guideline standard, applies it to the documented clinical facts, and explains whether the documented findings satisfy or fall short of the criteria.
Future Medical Care
Future medical care opinions project the specific treatment modalities — by type, frequency, and duration — that the claimant is likely to require over their remaining life expectancy, based on the documented diagnosis, treatment trajectory, and the published natural history for the relevant condition. In cases involving spinal cord stimulation, intrathecal drug delivery, or CRPS, the future care projection often represents the largest single component of economic damages, making the clinical precision of the IME physician's opinion directly consequential to case value. For the framework governing future care projections in pain management litigation, see the future medical care review service page.
Maximum Medical Improvement
MMI determination evaluates whether the claimant's condition has stabilized to the point where further active treatment is unlikely to produce material clinical improvement, or whether the condition remains in an active recovery phase. An MMI opinion distinguishes between curative treatment — aimed at further functional recovery — and palliative ongoing care that manages symptoms without altering the underlying condition. Both categories can be medically appropriate; MMI status determines how future care projections are framed and what damages categories are available.
Functional Impairment
When functional capacity is a contested issue — in disability cases, return-to-work disputes, or cases involving catastrophic injury — the IME physician assesses the clinical basis for claimed limitations. Physical examination findings including range of motion, strength testing, sensory examination, and observed gait and functional behavior provide objective data points that either support or call into question the functional limitations described in the treating record. For the full clinical methodology that underlies a pain management functional impairment evaluation, see the article on how pain management experts objectively evaluate pain. Documented functional impairment from an IME is also a recognized evidentiary bridge for pain and suffering and other non-economic damages claims — see the article on functional anchors for subjective pain complaints.
Records Needed for a Comprehensive Pain Management IME
The depth and defensibility of a pain management IME opinion depends directly on the completeness of the records provided. Attorneys should assemble the following materials before retention — incomplete records at intake produce opinions with qualification caveats that can be exploited at deposition.
- Complete treating records from all providers: Not only the pain management specialist, but primary care, physical therapy, orthopedic, neurosurgery, neurology, psychiatry or psychology, and any emergency department or urgent care records from the period surrounding the incident.
- Diagnostic imaging with radiology read reports: X-rays, MRI, CT, and bone scan studies — with the radiologist's formal written report for each study, not imaging alone. The IME physician's imaging interpretation must be reconciled with the radiologist's read.
- Operative and procedure reports: Surgical reports for any procedures performed before or after the incident, including interventional pain procedures (injection records, ablation reports, implant operative notes, and programming records for devices).
- Physical and occupational therapy records: Serial therapy notes documenting functional status, pain behavior, and functional progress or plateau over time — relevant to both causation and future care projections.
- Pharmacy records: A complete medication history documenting the timeline, dosing, and prescribing patterns for all pain-related medications. Particularly important in opioid management disputes and in cases where treatment escalation is a necessity argument.
- Prior IME reports and expert designations: Any prior independent medical examination reports, defense expert reports, or expert opinions from related civil proceedings.
- Deposition transcripts of treating physicians: When available before the IME, treating physician deposition testimony can identify disputed clinical claims and sharpen the specific questions the IME physician needs to address.
- Employment and vocational records: When functional capacity, disability, or lost income is at issue — job descriptions, occupational demand records, and employer-reported attendance or accommodation records provide context for the functional impairment opinion.
Independent Medical Evaluation vs. Treating Physician Opinion
Attorneys frequently ask how a treating physician's opinion and an IME opinion differ in their evidentiary function at trial. Understanding these differences — and the predictable points of disagreement between them — is essential to building a cohesive expert strategy.
Structural Differences
The treating physician's records and testimony reflect real-time clinical decision-making: diagnoses established at the time of treatment, treatment decisions made under therapeutic obligation to the patient, and documentation generated for clinical purposes rather than litigation purposes. The IME physician, by contrast, reviews the complete record retrospectively, applies the specific medicolegal questions posed by the retaining attorney, and produces a report designed from the outset for use in litigation. This structural difference means the two opinion types are not simply competing answers to the same question — they are analytically distinct products serving different functions.
Strengths and Limitations
The treating physician has longitudinal knowledge of the patient — clinical context accumulated across months or years of care — that a single-examination IME physician cannot replicate. That longitudinal context is a genuine strength, particularly for progressive conditions like CRPS where the clinical evolution over time is itself part of the evidence. The limitation is that the treating physician's documentation may not address the specific medicolegal questions litigation requires, and the treating record may contain gaps, inconsistencies, or conclusions stated without the guideline-level specificity that admissibility standards in many jurisdictions now demand.
The IME physician can review the complete record — including records from all providers, not only the treating physician's own notes — and can apply explicit clinical standards (specialty society guidelines, Budapest Criteria, published necessity criteria) to the documented findings in a systematic way that is often absent from the treating record. The limitation is that the IME is a snapshot: a single examination at a single point in time, without the longitudinal clinical context the treating relationship provides.
Why Disagreements Occur
Disagreements between treating and IME physicians are not necessarily evidence that one physician is wrong. They frequently reflect genuine clinical uncertainty, different interpretive frameworks, different access to the full record, or different analytical questions being answered. The treating physician addressing whether to continue a given treatment and the IME physician addressing whether that treatment was medically necessary under a published guideline standard are not answering the same question — and their divergent conclusions can both be defensible.
Disagreements that reflect genuine documentation gaps — where the treating record does not record the examination findings required to support the treating diagnosis or the necessity criteria for the treatment rendered — are more clinically significant and are the category most likely to affect the outcome at trial. Identifying those gaps early, before expert disclosure, is one of the most strategic uses of a plaintiff-side IME review.
Plaintiff and Defense Use of IMEs
Pain management IMEs serve different but complementary strategic functions for plaintiff and defense counsel. Understanding both perspectives allows attorneys on either side to anticipate the other's approach.
Plaintiff Perspective
Plaintiff attorneys most commonly retain a pain management IME physician to confirm the treating diagnosis and causation opinion with an independent clinical foundation — particularly in cases where the treating physician's documentation is sparse, where the treating physician has a lien interest in the case outcome, or where the case involves a high-value implantable device whose necessity the defense is expected to challenge. A plaintiff IME review that proactively identifies documentation gaps before the defense IME is conducted allows those gaps to be addressed — with supplemental treating documentation, additional testing, or a more focused treating physician opinion — rather than discovered for the first time at deposition.
Defense Perspective
Defense counsel and insurance carriers retain IME physicians primarily to evaluate whether the treating diagnosis is supported by the Budapest Criteria or other applicable diagnostic standards, whether causation between the incident and the diagnosed condition is clinically defensible, whether treatment rendered met the necessity standard applicable to each procedure, and whether the future care projection is grounded in the claimant's actual clinical picture or is inflated beyond what the documented condition supports. A well-grounded defense IME opinion that specifically targets the weakest links in the treating record — documentation gaps in necessity criteria, mechanism-severity arguments in causation, or over-projected future care — is among the most consequential tools available to defense counsel in high-value pain management cases.
Mediation and Settlement
IME reports frequently drive settlement outcomes — particularly in cases where the parties' medical positions diverge sharply. A detailed, guideline-grounded IME opinion that either supports or challenges the treating record's narrative provides the mediator and the opposing party with a specific, clinically documented basis for evaluating the medical risk in the case. Vague or conclusory IME reports that state clinical conclusions without the underlying reasoning are less effective settlement tools, because they invite equally vague rebuttal rather than a specific clinical engagement with the disputed questions.
Trial
At trial, the IME physician's report and testimony must satisfy the admissibility standard of the applicable jurisdiction — Daubert or Frye in federal and many state courts, Evidence Code §§ 801-802 and the Sargon reliability standard in California courts, and comparable standards in Texas Chapter 74 matters. For a full discussion of how these standards apply to pain management expert testimony, see the California Pain Management Expert Witness Guide and the Texas pain management expert witness resources.
Common Pain Management Conditions Evaluated During IMEs
Pain management IMEs cover the full spectrum of conditions, procedures, and disputes that arise in chronic pain litigation. The following conditions represent the most frequently evaluated in Dr. Dardashti's practice.
- Complex Regional Pain Syndrome (CRPS / RSD): Budapest Criteria documentation review, causation from trauma or surgery, mechanism-severity analysis, treatment necessity, SCS candidacy, and long-term future care projection. CRPS is among the most contested diagnoses in pain management litigation and requires an IME physician with direct clinical experience evaluating Budapest Criteria findings at examination. For a comprehensive discussion of CRPS litigation issues, see the CRPS Expert Witness Guide.
- Post-Laminectomy Syndrome: Persistent spinal pain following disc surgery, decompression, or fusion — including causation linking the original accident to the surgical indication, standard of care for post-surgical pain management, and future care involving SCS or ongoing interventional management.
- Peripheral Nerve Injury: Electrodiagnostic correlation, functional deficits in the distribution of the injured nerve, causation from the mechanism of trauma, and the appropriateness of neuromodulation or surgical treatment for refractory neuropathic pain.
- Amputation and Phantom Limb Pain: Residual limb pain, phantom neuropathic pain, and the medical necessity of long-term pharmacological and neuromodulatory management in catastrophic injury cases.
- Spinal Cord Stimulation Disputes: Trial period documentation adequacy, psychological clearance, permanent implantation necessity, battery replacement intervals, revision probability, and projected lifetime device costs in future care calculations.
- Intrathecal Pump Therapy: Candidacy criteria, dosing disputes, pump and catheter replacement schedules, complication evaluation, and future care projections for implanted drug delivery systems.
- Epidural Steroid Injection Disputes: Imaging correlation with the injected level, necessity documentation for each injection in a series, frequency disputes, and fluoroscopic guidance standard of care analysis.
- Radiofrequency Ablation Disputes: Diagnostic medial branch block sequencing adequacy, documented pain relief threshold, correct anatomic levels, and future necessity for repeat RFA procedures as ablated nerves regenerate.
Scope of IME Engagements
IME engagements are scoped at intake to the specific questions the case requires. A records-only review may be sufficient for early case evaluation — to assess the strength of the treating physician's documentation before investing in a full examination and report. A combined records review and physical examination adds contemporaneous objective findings for cases where current clinical status is contested. A focused rebuttal opinion, addressing only the specific arguments raised in an opposing expert's report, is available when the full IME work has already been done and only a targeted response is needed.
For matters also requiring deposition and trial testimony, the IME engagement can be structured to include expert witness services from the outset. For cases requiring only a written causation analysis without examination, see the causation analysis service. For cases where the primary need is a physician-level review of the existing records and a written opinion without scheduling a physical examination, see the medical record review service.
How to Request an IME
Contact Expert Medical Services LLC with the case summary, the specific opinion areas to be addressed, the format of the engagement (records review, records review plus examination, or rebuttal opinion), and any relevant deadlines — including expert disclosure cutoffs, deposition dates, and mediation or trial dates. A preliminary record set is helpful for case intake, though the complete record set should be provided before the examination is scheduled.
Attorneys in California should review the California Pain Management Expert Witness Guide for a discussion of how IME opinions intersect with Evidence Code admissibility standards and MICRA's effect on future care opinion significance in malpractice cases. For cases venued in Texas, the Texas pain management expert witness page covers Chapter 74 and related procedural requirements.
Related Services & Expertise
Causation Analysis
Linking mechanism of injury to diagnosis — causation opinions for personal injury and malpractice matters.
Future Medical Care Review
Projecting ongoing treatment costs once IME findings establish the clinical picture.
Medical Necessity Review
Physician-level necessity analysis for past and projected treatment disputes.
Expert Witness — California
Deposition and trial testimony in California state and federal court.
CRPS Expert Witness Guide
Budapest Criteria, causation, future care, and common attorney mistakes in CRPS litigation.
California Expert Witness Guide
Evidence Code §§ 720, 801-802, Sargon, MICRA, and IME practice for California attorneys.
FAQ
IME — Common Attorney Questions
- An IME provides an objective, independent assessment of a claimant's condition by a physician who has no prior treating relationship with the individual. In litigation, IMEs are used to evaluate the diagnosis, causation, extent of injury, treatment appropriateness, and future medical needs from a neutral clinical perspective. The IME report is then available for use in settlement negotiations, motions, depositions, and trial.
- Yes. A board-certified pain management physician is frequently the appropriate expert for IMEs involving chronic spinal pain, neuropathic pain, CRPS, post-laminectomy syndrome, interventional procedure disputes, and implantable device cases. Pain management subspecialty training and active clinical experience with the procedures and conditions at issue — rather than general medical credentials alone — determine whether the IME physician is adequately qualified to address the specific clinical questions in the case. In California and most jurisdictions, expert qualification for IME purposes requires special knowledge of the subject at hand, which a board-certified, actively practicing pain management physician satisfies for the conditions within that specialty.
- No. An IME can be conducted as either a records-only review or as a combined records review with physical examination, depending on the questions to be addressed and the strategic needs of the case. A records-only review produces opinions grounded entirely in the treating record — appropriate when the claimant's current physical presentation is not in dispute, when examination findings are unlikely to change the opinion, or when the retaining party prefers not to introduce a contemporaneous examination into the record. A records review with examination adds objective, current clinical findings from an independent examiner, which can be particularly important in CRPS, functional impairment, and MMI disputes where contemporaneous physical findings are central to the contested questions.
- Yes. Causation is one of the most frequently requested IME opinion areas in personal injury pain management cases. The IME physician reviews the mechanism of injury, the pre-existing medical history, the temporal relationship between the incident and the documented clinical findings, and any competing explanations offered by the defense or treating team. The causation opinion is expressed to the applicable legal standard — typically a reasonable degree of medical probability — and should identify the specific clinical record evidence and the specific analytical reasoning supporting each causation conclusion rather than stating a bare conclusion.
- Yes. Future medical care is a standard IME opinion area in cases involving chronic pain conditions, implantable devices, and long-term treatment needs. The IME physician projects the specific treatment modalities likely to be required — by type, frequency, and duration — based on the claimant's documented clinical condition, their treatment response to date, and the published literature on the expected management course for the relevant diagnosis. In high-value cases involving spinal cord stimulation, intrathecal drug delivery, or CRPS, the future medical care projection is often the largest single damages component and warrants the most granular clinical analysis.
- A treating physician's primary obligation is to the patient's care — the treating record reflects clinical decision-making in real time, not a comprehensive medicolegal analysis. An IME physician's obligation is to the accuracy of the medical opinion on the specific questions posed. The IME physician reviews the complete record — including records the treating physician may not have seen — conducts a structured examination, and prepares a written report that addresses each medicolegal question with citation to the clinical record and the applicable clinical standards. These structural differences mean that a treating physician's testimony and an IME report address different analytical questions and serve different purposes, even when they reach the same clinical conclusions.
- Dr. Dardashti evaluates the full range of chronic pain conditions encountered in personal injury and malpractice litigation — including CRPS/RSD, post-laminectomy syndrome, peripheral nerve injury, chronic spinal pain with radiculopathy, neuropathic pain, and conditions requiring interventional management such as spinal cord stimulation, intrathecal drug delivery, epidural steroid injections, and radiofrequency ablation. His evaluations address diagnosis, causation, medical necessity of past and future treatment, MMI, and functional impairment.
- The IME report addresses the specific questions posed by the retaining attorney. Standard opinion areas include: (1) whether the diagnosis is supported by the clinical evidence and examination findings; (2) whether the condition is causally related to the subject incident or pre-existing; (3) whether treatment rendered was medically necessary and within the standard of care; (4) whether the claimant has reached maximum medical improvement; (5) the nature, scope, and projected cost of future medical care; and (6) functional limitations relevant to damages. The report is structured for litigation use — with citation to the clinical record and the applicable specialty society guidelines supporting each conclusion.
- A comprehensive IME requires the complete treating record from all providers — not only the pain management specialist, but primary care, physical therapy, orthopedic, neurology, and any surgical providers. Attorneys should also provide all diagnostic imaging with the radiologist's formal read reports, operative and procedure reports, pharmacy records, prior IME or expert reports, deposition transcripts of treating physicians, and — where employment records are relevant to disability or future wage claims — occupational history documentation. The completeness of the records provided directly determines the depth and defensibility of the IME opinion. Gaps in the record that the attorney is aware of before retention should be identified at intake, so the IME physician can address them explicitly rather than discovering them mid-review.
- The examination itself typically requires 45 to 90 minutes depending on the clinical complexity and the scope of the evaluation. Record review and report preparation add additional time, which varies with the volume of records and the number of opinion areas requested. Attorneys should allow adequate lead time before deposition and trial deadlines — retaining the IME physician at least 60 to 90 days before the expert disclosure deadline is advisable in complex cases involving CRPS, post-laminectomy syndrome, or high-value future care projections.
- Yes. MMI determination is a standard IME opinion area in personal injury matters. The IME physician evaluates whether the claimant's condition has stabilized to the point where further active treatment is unlikely to produce material clinical improvement, or whether the condition remains in a phase of active recovery. An MMI opinion distinguishes between palliative ongoing care — treatment that manages symptoms without improving the underlying condition — and curative treatment aimed at further functional recovery. Both can be medically necessary; MMI status determines which category the projected future care falls into.
- Yes. Dr. Dardashti accepts retention for both plaintiff and defense IMEs. On the defense side, the IME typically evaluates whether the diagnosis and claimed causation are supported by the treating record, whether treatment rendered was medically necessary, and whether future care projections are clinically justified. On the plaintiff side, an independent review can confirm the adequacy of the treating physician's documentation and the clinical support for each opinion before the case reaches expert disclosure — identifying any documentation gaps early enough to address them strategically. The IME physician's obligation in both contexts is to an accurate opinion, not to the result the retaining party prefers.
- Report turnaround depends on the complexity of the case, the volume of records, and the number of opinion areas addressed. For most standard pain management IMEs, written reports are delivered within two to three weeks of examination completion. Complex cases involving extensive records, multiple opinion areas, or high-value future care projections may require additional time. Attorneys with specific deadline constraints — including expert disclosure deadlines, deposition scheduling, or mediation dates — should communicate those deadlines at the time of retention so the engagement timeline can be structured accordingly.
- Yes. Dr. Dardashti conducts IMEs and provides written expert opinions for cases venued in California and nationally. Records-only reviews are available for any jurisdiction. Physical examination IMEs outside California require confirmation of scheduling logistics and availability. Contact the office at 805-267-9308 to discuss your case, confirm availability, and determine the appropriate engagement format.
Request an Independent Medical Evaluation
Contact Expert Medical Services LLC to schedule an IME or request a record review opinion. Availability confirmed after case intake.