Nationwide Pain & Injury Medical Expert Witness
Cauda Equina Syndrome Expert Witness
Pain management evaluation of cauda equina syndrome — chronic neuropathic pain sequelae, causation, standard of care, neuromodulation, and future medical care in complex personal injury and malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Condition
- Cauda Equina Syndrome (CES)
- Classification
- Catastrophic Spinal Neurologic Injury
- Specialty
- Pain Management & Anesthesiology
- Evaluation Areas
- Causation, Standard of Care, Neuropathic Sequelae, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Cauda Equina Syndrome in Pain Management Review
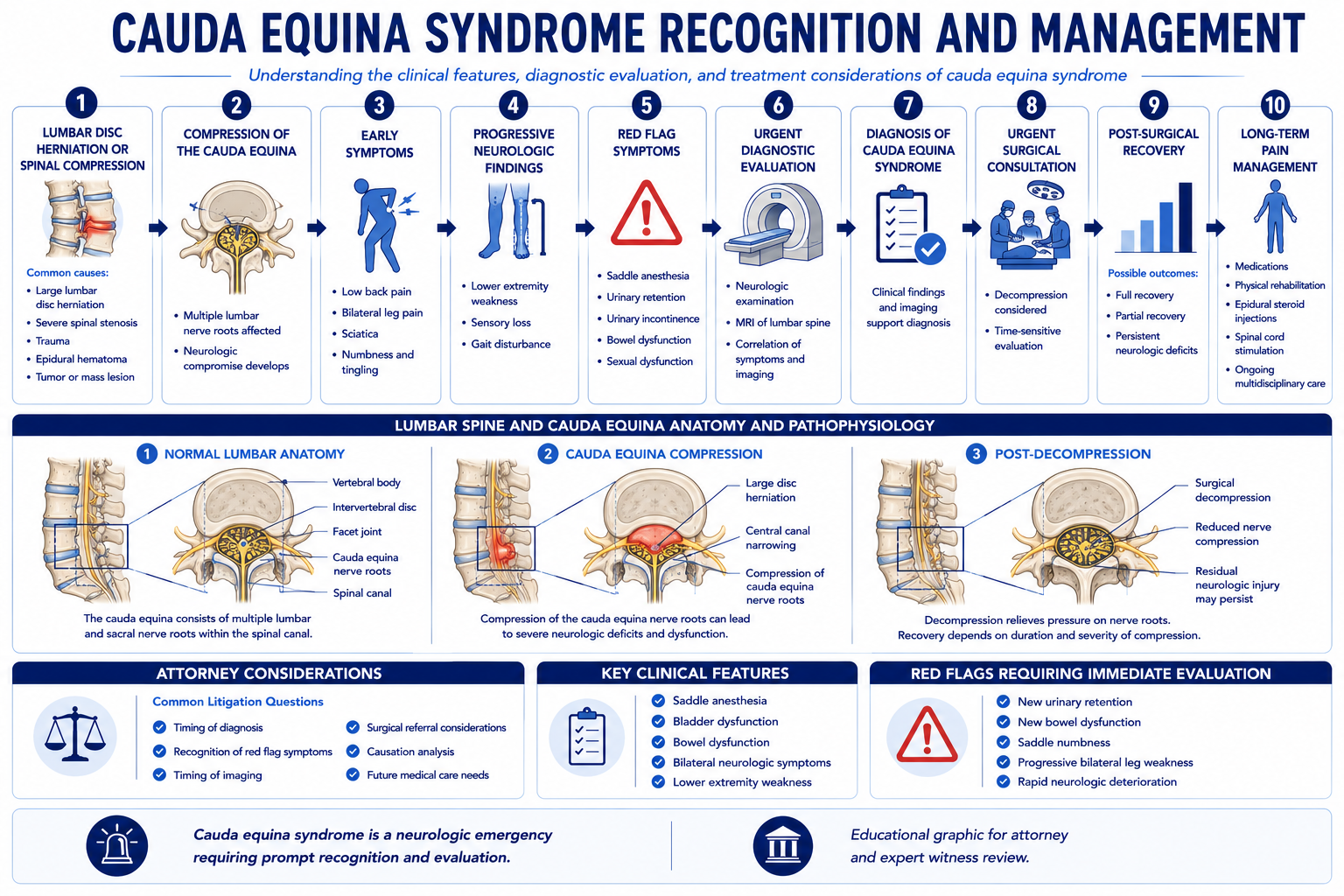
Cauda equina syndrome (CES) is one of the most serious neurological conditions in spinal medicine — a compression of the lumbar and sacral nerve roots within the spinal canal that produces the characteristic constellation of saddle anesthesia, bladder and bowel dysfunction, and bilateral lower extremity weakness or pain. CES is predominantly a neurosurgical emergency, and the questions of surgical timing, decompression adequacy, and neurosurgical standard of care are addressed by spine surgery or neurosurgery experts. The pain management evaluation in CES litigation addresses a different and equally important set of issues: the chronic neuropathic pain sequelae that develop after the acute event and surgical treatment, the appropriateness of the ongoing pain management, and the long-term future care requirements.
In the litigation context, CES cases present across both personal injury and medical malpractice frameworks. In personal injury matters, a traumatic event — motor vehicle collision, workplace injury, or fall — produces the disc herniation or spinal injury that causes CES, and the chronic pain sequelae become part of the damages analysis alongside the neurological deficits. In malpractice matters, claims typically arise from alleged delays in diagnosis or surgical decompression — issues requiring surgical experts — but the post-decompression pain management may also be independently at issue when chronic pain was not appropriately recognized and managed.
Expert review from a pain management perspective is grounded in the clinical record, the available imaging, and the scope of questions defined by retaining counsel. All opinions are case-specific and are delivered within reasonable medical probability.
What Is Cauda Equina Syndrome?
The cauda equina (Latin: "horse's tail") is the collection of lumbar, sacral, and coccygeal nerve roots that descend below the conus medullaris — the terminal end of the spinal cord, typically at the L1–L2 vertebral level — and travel through the lumbar spinal canal to exit at their respective neural foramina. These nerve roots are responsible for motor function and sensation in the lower extremities, sensation in the perineum and saddle region, and voluntary control of bowel and bladder function through the sacral nerve roots.
Cauda equina syndrome occurs when these nerve roots are compressed within the spinal canal at a degree and duration sufficient to produce neurological dysfunction. The most common cause is a large central or paracentral lumbar disc herniation — most often at L4–L5 or L5–S1 — that occupies sufficient volume in the spinal canal to compress multiple nerve roots simultaneously. Other causes include: lumbar spinal stenosis with superimposed acute disc herniation; epidural hematoma following spinal surgery or anticoagulation; epidural abscess from infection; primary or metastatic spinal tumors; and vertebral fracture from trauma producing bony retropulsion into the canal. In each case, the compressive pathology is visible on MRI of the lumbar spine, which is the definitive imaging study for CES diagnosis.
The classic clinical triad of CES consists of: saddle anesthesia — reduced or absent sensation in the perianal, perineal, and genital regions corresponding to the S2–S4 dermatomes; bladder dysfunction — typically urinary retention with reduced bladder sensation, which is the most consistent and diagnostically specific finding; and bilateral lower extremity neurological symptoms — which may include weakness, sensory loss, or pain in the legs and feet in the distribution of the compressed lumbar and sacral nerve roots. Bowel dysfunction and sexual dysfunction are also common components of the full CES syndrome.
The clinical recognition of CES — and the clinical record documenting its presentation — is the foundation for all subsequent litigation issues, whether in personal injury (establishing the neurological injury caused by the traumatic event) or malpractice (establishing the clinical state at the time the diagnosis was or should have been made). From a pain management perspective, the initial neurological presentation determines the nerve root injury pattern and therefore informs the expected distribution and character of chronic pain sequelae.
Complete vs. Incomplete Cauda Equina Syndrome
The most clinically and medico-legally significant classification in CES is the distinction between complete and incomplete presentations based on bladder function at the time of initial evaluation:
- › Incomplete CES (CESI) — The patient experiences urinary symptoms — difficulty initiating urination, incomplete bladder emptying, altered bladder sensation — but retains some degree of voluntary bladder control. Saddle hypoesthesia may be present but partial rather than complete. CESI represents a clinical window during which surgical decompression may prevent progression to complete neurological deficit. Prognosis for bladder and bowel function recovery in CESI is generally better than in complete CES, though residual deficits are common.
- › Complete CES (CESC) — The patient presents with painless urinary retention — complete loss of bladder sensation and voluntary control. Saddle anesthesia is typically complete. CESC represents a more advanced stage of nerve root compression and carries a worse prognosis for recovery of bladder, bowel, and sexual function. Even following timely surgical decompression, residual neurological deficits — including persistent bladder and bowel dysfunction — are common in CESC.
The CESI/CESC classification at presentation is a critical data point for future care projections. Patients presenting with CESC face higher rates of permanent bladder and bowel dysfunction requiring lifelong management, and typically experience more severe and persistent chronic neuropathic pain. The expected chronic pain trajectory — including the likelihood of refractory neuropathic pain requiring advanced treatment — differs materially between the two presentations.
From a pain management perspective, the CESI/CESC distinction informs the prognosis analysis. A patient who presented with CESC and undergoes surgical decompression faces a higher probability of persistent chronic neuropathic pain in the perineal, perianal, and lower extremity distribution — a longer and more treatment-intensive chronic pain course. This clinical reality must be reflected in a defensible future care projection. The absence of documentation of bladder function status at initial presentation — whether CESI or CESC — is a recurring documentation gap in malpractice matters where the timeline and severity of the acute presentation are contested.
Chronic Pain Following Cauda Equina Syndrome
Persistent chronic pain is one of the most significant long-term consequences of cauda equina syndrome, and it is the primary domain of the pain management evaluation in CES litigation. The clinical literature consistently documents that a substantial proportion of CES patients — estimated between 50% and 80% in various series — experience persistent pain following surgical decompression, and that chronic pain significantly affects quality of life, functional capacity, and return to pre-injury activities.
The chronic pain patterns following CES are heterogeneous and may involve multiple pain generators simultaneously:
- › Bilateral radicular lower extremity pain — Pain radiating from the lumbar region into the lower extremities in a dermatomal pattern consistent with the compressed nerve roots. The most common distributions involve the L4, L5, and S1 nerve root territories — pain along the lateral thigh and calf (L5), the posterior thigh and calf (S1), and the medial thigh and knee (L4). The radicular pain following CES may have both neuropathic features (burning, electric, shooting) and mechanical features (worsening with loading and walking). The radicular pain component may partially respond to epidural steroid injections when it reflects ongoing nerve root inflammation, or may be refractory to injection treatment when it reflects established nerve root injury and central sensitization.
- › Perineal and perianal neuropathic pain — Injury to the sacral nerve roots (S2–S4) — which provide sensation to the perianal, perineal, and genital regions — produces a distinct and often particularly distressing neuropathic pain syndrome in the saddle distribution. This pain is frequently described as burning, pressure-like, electric, or hypersensitive to contact, and it may be worsened by sitting, defecation, or urination. Perineal neuropathic pain is among the most treatment-resistant features of post-CES chronic pain and is specifically relevant to future care projections involving advanced neuromodulation.
- › Lower back pain — Axial lower back pain from the disc herniation level, the surgical site, post-surgical epidural fibrosis, and any secondary adjacent segment degeneration from prior fusion surgery (when performed). Mechanical lower back pain may have facet-mediated components amenable to medial branch block and radiofrequency ablation, as well as post-surgical components similar to post-laminectomy syndrome.
- › Central sensitization — In patients with prolonged pre-surgical nerve root compression or with persistent post-surgical pain, central sensitization — a state of amplified central nervous system pain processing — can develop and perpetuate pain independent of ongoing structural pathology. Central sensitization explains the clinical phenomenon of pain that persists and may intensify after technically successful decompression, and it affects both the prognosis for spontaneous improvement and the likelihood of response to further structural interventions. Its presence is relevant to both the treatment planning and the future care analysis.
- › Neuropathic bladder and bowel pain — Dysfunction of bladder and bowel — incomplete emptying, urgency, incontinence — can itself produce pain associated with the voiding dysfunction, particularly in patients with urge incontinence or in those performing intermittent self-catheterization for urinary retention. This component of the pain syndrome requires urological co-management and is distinct from the neuropathic pain in the lower extremity and perineal distribution.
The combination and relative severity of these pain patterns is highly individual and requires documentation in contemporaneous clinical records to be medico-legally defensible. A treating pain management physician who does not distinguish between these pain generators and document their individual clinical characteristics may not be providing — or documenting — care consistent with the standard for complex post-CES pain management.
Pain Management Evaluation
A complete pain management evaluation for a CES patient addresses both the acute and chronic pain dimensions of the clinical picture. The evaluation should document the character, distribution, and intensity of each pain component; correlate the pain pattern with the documented nerve root injury from the imaging and operative record; assess functional status and activity limitations; and identify any psychological comorbidities relevant to treatment planning. Pain management in post-CES patients follows a graduated approach:
- › Pharmacological management — First-line pharmacological treatment for post-CES neuropathic pain includes calcium channel modulators (gabapentin, pregabalin) and tricyclic antidepressants or serotonin-norepinephrine reuptake inhibitors (duloxetine). These agents address the neuropathic pain character of post-CES pain more directly than opioids and are the appropriate first-line pharmacological approach. Anti-inflammatory agents may be appropriate for inflammatory components in the acute post-surgical period. Long-term opioid management may be considered in selected patients with severe persistent pain who have not responded to non-opioid neuropathic agents, but requires a complete documentation framework including informed consent, prescription monitoring program compliance, urine drug screening, and periodic reassessment of functional goals.
- › Interventional procedures — Epidural steroid injections — transforaminal or interlaminar — may be appropriate for post-decompression radicular pain components when the pain distribution and clinical findings support ongoing nerve root irritation or inflammation at a specific level. The documentation of each procedure — the specific level targeted, the approach, the documented response, and the basis for repeat procedures — is subject to medical necessity review. Sacral nerve blocks or targeted transforaminal injections at the sacral foramina may be considered for perineal and perianal neuropathic pain from sacral nerve root injury.
- › Physical therapy and rehabilitation — Physical therapy addressing lower extremity strengthening, gait rehabilitation, and functional mobility is an important component of post-CES management. Pelvic floor physical therapy — performed by a therapist with specialized pelvic floor training — addresses the bowel and bladder dysfunction components and may reduce associated pelvic pain. Occupational therapy addresses adaptive function and activities of daily living when functional limitations are significant.
- › Multidisciplinary pain rehabilitation — When psychological comorbidities — depression, anxiety, catastrophizing — are identified as significant contributors to the pain and disability picture, referral to a multidisciplinary pain program incorporating psychology, physical therapy, and pain medicine is consistent with the standard of care. The treating pain management record should document whether psychological comorbidities were assessed and whether referral for psychological support was considered.
- › Neuromodulation — When conservative and conventional interventional management fails to provide adequate relief, escalation to spinal cord stimulation or peripheral nerve stimulation may be considered for appropriate candidates. For post-CES patients in whom the bilateral and perineal neuropathic pain distribution is not adequately covered by standard SCS, intrathecal drug delivery may be considered as an alternative or adjunct neuromodulation pathway. The pre-implant evaluation sequence — documented conservative care failure, psychological screening, and successful trial stimulation — is the same as for all SCS indications.
Future Medical Care Considerations
Future medical care for post-CES neuropathic pain is one of the most significant components of damages analysis in CES personal injury and malpractice litigation. The pain management component of future medical care must be grounded in the specific clinical course documented in the treating record — the severity of the initial injury, the degree of neurological recovery, and the character of the post-surgical pain syndrome — rather than in generic CES templates.
- › Ongoing pharmacological management — Neuropathic agents (gabapentinoids, SNRIs, tricyclics) and any analgesics currently in use with documented clinical benefit constitute recurring future care costs. The projected medications and dosages should reflect those currently prescribed with documented response. Speculative projection of future medications not supported by the current treating course are subject to challenge.
- › Interventional procedures — Epidural steroid injections and other targeted pain procedures that have been part of the treating course and are projected to continue may be included as recurring future care. The frequency of projected procedures should be based on the documented treatment history — the treating physician's injection schedule and clinical response — not a maximum-frequency template.
- › Rehabilitation — Projected physical therapy and pelvic floor therapy requirements should reflect the documented rehabilitation course and the treating physician's assessment of ongoing functional limitations requiring therapeutic support. Not all CES patients require indefinite ongoing physical therapy — the projection should be grounded in the actual clinical trajectory.
- › Spinal cord stimulation — Where the clinical record and current treatment trajectory support a future SCS need — particularly in patients with severe refractory perineal or lower extremity neuropathic pain who have completed an adequate conservative care trial — the future care projection should include trial stimulation, permanent implantation with device-specific cost documentation, battery replacement cycles at published intervals, revision procedures at published complication rates, and ongoing programming visits. The clinical basis for projecting SCS must be addressed before including it as a future care item. A patient still in the early post-surgical period without completed conservative management is not yet an SCS candidate, and projecting SCS for that patient would be premature without appropriate clinical caveats.
- › Defense review of life care plans — Defense review of a plaintiff CES future care projection addresses whether each proposed pain management item is clinically supported by the documented post-surgical course, whether the severity of the initial injury (CESI vs. CESC) supports the projected intensity of future care, whether SCS necessity is established by the available record, and whether projected costs reflect the plaintiff's geographic treatment market. The absence of adequate treating records — or treating records that do not document pain severity and treatment response — weakens both plaintiff and defense future care positions.
Spinal Cord Stimulation and Neuromodulation
Spinal cord stimulation is an established treatment option for refractory neuropathic pain following cauda equina syndrome, and it arises in CES litigation both as a past treatment whose necessity is disputed and as a projected future care item in personal injury damages analysis. SCS delivers electrical impulses through epidurally placed thoracic leads to modulate pain signaling in the dorsal columns, and is particularly effective for lower extremity neuropathic pain with a dermatomal or nerve root distribution — exactly the predominant pain pattern in post-CES radicular pain.
The perineal and perianal neuropathic pain from sacral nerve root injury — one of the most distinctive and treatment-resistant features of CES — presents a more complex neuromodulation challenge. Conventional spinal cord stimulation with thoracic lead placement may provide coverage for lower extremity distribution pain, but targeted sacral nerve root stimulation or dorsal root ganglion (DRG) stimulation at the affected sacral levels may be more appropriate for the perineal pain component. In cases where SCS is being projected as future care in a CES patient with significant perineal neuropathic pain, the neuromodulation approach should specify the evidence base for the selected modality.
CES patients may also develop post-decompression changes consistent with post-laminectomy syndrome — epidural fibrosis, adjacent segment disease, or pseudarthrosis following fusion surgery — in which case the SCS indication and evidence base aligns with the broader post-laminectomy syndrome evidence. In some patients, the post-CES pain syndrome may meet criteria for a CRPS Type II diagnosis — CRPS is a recognized complication of significant nerve root injury and carries an independent SCS indication with strong randomized trial evidence.
The pre-implant evaluation requirements for SCS in post-CES patients follow the same sequence as all SCS indications: documented failure of appropriate conservative management, psychological screening, and a successful trial stimulation period with contemporaneous documentation of pre-trial and post-trial pain scores demonstrating at least 50% improvement. In post-CES patients with significant bladder and bowel dysfunction, sacral neuromodulation may also be relevant for the bladder and bowel symptoms — but this is a urological indication reviewed by urology, not pain management.
Causation Analysis — Pain Management Perspective
Causation analysis from a pain management perspective in CES cases operates on two levels. The first — whether the subject event produced the disc herniation or spinal injury that caused CES — is primarily a neurosurgical or spinal orthopedic causation question, though the pain management expert may provide a supporting opinion regarding the mechanism's consistency with the documented clinical presentation. The second — whether the chronic pain sequelae documented in the post-surgical course are causally related to the nerve root compression from CES — is the primary pain management causation question.
The pain management causation analysis addresses:
- › Injury chronology — Whether the temporal sequence of the traumatic event, the onset of CES symptoms, the surgical decompression, and the post-surgical chronic pain onset is internally consistent with the expected clinical course of CES. The timeline from injury to CES presentation to chronic pain establishment should be documented and examined for consistency.
- › Symptom progression — Whether the chronic pain symptoms documented in the post-surgical treating record are consistent with the expected progression from nerve root compression and surgical recovery. The post-CES pain pattern — bilateral lower extremity radicular pain, perineal and perianal neuropathic pain — should correspond anatomically to the nerve roots identified on imaging and operative findings as the site of compression.
- › Objective findings — MRI imaging identifying the compressive pathology and its relationship to the nerve roots; post-surgical imaging documenting decompression adequacy; electrodiagnostic studies if performed, which may document nerve root denervation consistent with the level and side of compression; and clinical examination findings including sensory testing in the saddle distribution, lower extremity reflexes, and motor strength.
- › Pre-existing spinal conditions — The presence of pre-existing lumbar disc disease, prior lumbar surgeries, or prior episodes of lower back or leg pain does not preclude accident-related causation, but requires a specific analysis of whether the subject event produced new structural injury, aggravated a symptomatic pre-existing condition, or accelerated an asymptomatic degenerative process to become clinically symptomatic requiring surgery. This apportionment analysis is a recurring element of personal injury CES cases involving adults with prior imaging or prior back symptoms.
Standard of Care Considerations — Pain Management Scope
The pain management standard of care in CES matters addresses the obligations of the pain management physician responsible for the post-decompression chronic pain — not the surgical timing, decompression adequacy, or neurosurgical standard of care, which are outside this scope and require surgical expertise. Expert review from a pain management perspective evaluates whether the chronic pain management provided to the post-CES patient met the standard of care for a reasonably competent pain management specialist. For the clinical examination methodology — including neurological assessment, functional evaluation, and validated outcome instruments — that defines the standard-of-care expectation for post-CES pain evaluation, see the article on how pain management experts objectively evaluate pain.
- › Comprehensive initial pain evaluation — The initial pain management evaluation of a post-CES patient should obtain the operative report and pre- and post-surgical imaging, document the specific pain patterns present (radicular, perianal, axial), correlate the pain distribution with the documented nerve root injury, and formulate a treatment plan matched to the identified pain generators. An evaluation that proceeds directly to interventional procedures without this clinical characterization does not meet the standard for complex post-CES pain assessment.
- › Appropriate pharmacological approach — Initiating neuropathic-specific pharmacological agents — gabapentinoids, SNRIs, tricyclics — as the foundation of post-CES pain management is consistent with the current standard of care for neuropathic pain. An opioid-centric approach without an adequate trial of neuropathic-specific agents is below the standard for neuropathic pain management regardless of pain severity. Opioid management, when used, must be accompanied by appropriate monitoring documentation.
- › Graduated escalation — The treatment plan should follow an appropriate escalation from conservative pharmacological and rehabilitative management through interventional procedures and, where indicated, advanced neuromodulation. Premature escalation to high-cost or high-risk procedures without documented failure of appropriate conservative care is a medical necessity and standard of care concern, as is failure to escalate when conservative measures have demonstrably failed and the clinical record supports a more advanced approach.
- › Referral and follow-up obligations — A spine surgeon or neurosurgeon who discharges a post-CES patient without arranging follow-up or referral for the chronic pain dimensions of the clinical picture — and who does not refer to pain management when persistent neuropathic pain is documented in the post-operative course — may have a referral standard of care issue. The appropriate timing of post-surgical pain management referral in CES depends on the clinical course, but persistent radicular or perineal neuropathic pain beyond the expected post-surgical recovery window — without pain management evaluation — is a documented standard of care concern.
- › Documentation adequacy — The pain management record should document pain severity using validated scales, the character and distribution of pain, the response to each treatment modality, functional status over time, and the rationale for treatment changes. Documentation that fails to capture these elements — particularly when future care projections and standard of care are contested — limits the defensibility of both the treating physician's care and the expert's opinion.
Common Litigation Issues
CES cases in litigation — whether personal injury or malpractice — consistently involve a defined set of recurring disputes that the pain management expert is frequently asked to address:
- › Causation of chronic neuropathic pain — Whether the chronic pain documented in the post-surgical record is a recognized consequence of the cauda equina compression, or whether it is attributable to pre-existing conditions, post-surgical changes unrelated to CES, or another cause. The anatomical consistency of the pain pattern with the documented compression level is central to this analysis.
- › Future medical care disputes — The most significant single issue in high-value CES personal injury cases. Disputes center on whether future pain management needs are clinically supported, whether SCS is an appropriate future care item, whether projected frequencies and durations are grounded in the clinical record, and whether costs reflect current market pricing. The clinical severity classification (CESI vs. CESC) and the documented post-surgical pain course are the primary anchors for defensible future care opinions.
- › Functional impairment claims — The functional consequences of post-CES pain — reduced ambulation, sitting intolerance from perineal pain, bladder and bowel management demands, sleep disruption — affect vocational capacity and activities of daily living. These functional limitations require independent documentation in the clinical record through functional capacity evaluations, treating physician functional assessments, and therapy records. Pain management expert review addresses whether the documented functional limitations are consistent with the clinical severity of the pain syndrome, not whether the patient's self-reported limitations are credible.
- › Neuromodulation necessity and cost — Whether SCS is a medically indicated future care item in a given CES patient depends on whether the refractory pain pattern is consistent with an established SCS indication, whether the conservative care trial has been completed, and whether the clinical trajectory supports a reasonable probability of SCS in the patient's future. Defense review challenges SCS projections on the grounds of inadequate conservative care trial, premature escalation, or absence of a documented indication for neuromodulation.
- › Medical necessity of treatment rendered — Whether the volume, type, and frequency of pain management treatment provided is consistent with the documented clinical severity and course. Insurers and defense counsel frequently dispute the medical necessity of extensive treatment in CES cases on the basis of documentation gaps, absence of validated outcome measures, or failure to document treatment response before proceeding to the next treatment level.
- › Pre-existing degenerative spinal disease — CES most commonly results from a large disc herniation superimposed on a lumbar spine with pre-existing degenerative changes. Pre-existing disc degeneration is common and does not preclude accident-related causation, but requires a specific analysis distinguishing between the traumatic component and the degenerative baseline. Apportionment analysis for future care — particularly for projected spinal pain management costs — must address what proportion of the future care is attributable to the traumatic CES event versus natural degenerative progression.
Expert Witness Review Process
A complete pain management expert review in a CES case requires a specific set of records. The scope of records needed depends on whether the engagement addresses causation of chronic pain, standard of care for post-decompression pain management, future medical care, or a combination defined in consultation with retaining counsel. Typical records include:
- › Initial presentation records — Emergency department records, urgent care records, or the initial treating physician's notes from the acute CES presentation, documenting the timeline of symptoms, the neurological examination findings (including saddle sensation, bladder function, bilateral lower extremity assessment), and the clinical classification as CESI or CESC
- › Imaging studies — MRI of the lumbar spine from the acute presentation identifying the compressive pathology (disc herniation level, disc fragment characteristics, canal stenosis measurement); post-surgical imaging documenting decompression adequacy; any subsequent imaging documenting post-surgical spinal changes or adjacent segment pathology
- › Operative reports — All operative reports from decompression surgery, documenting the surgical findings, the degree of nerve root compression encountered, the procedure performed, any intraoperative complications, and the post-decompression spinal assessment; any subsequent spinal surgical procedures
- › Complete treating pain management records — Initial evaluation notes, follow-up clinical notes, pre-procedure assessments, procedure records, post-procedure response documentation, and pharmacological management records from the beginning of the pain management relationship through the most recent encounter
- › Physical and occupational therapy records — Rehabilitation documentation from the post-surgical period, including pelvic floor therapy records where applicable, documenting treatment approach, patient response, and functional outcome measures
- › Urological and bowel management records — Records from urological evaluation and treatment for bladder dysfunction, including urodynamic studies if performed; bowel management records if separately documented
- › Electrodiagnostic records — EMG and nerve conduction studies if performed, documenting nerve root denervation consistent with the CES compression level and the post-decompression recovery trajectory
- › Prior lumbar spine records — Pre-injury lumbar spine records, prior imaging, and prior treating records establishing baseline spinal health, prior episodes of back or radicular pain, and any pre-existing disc disease or prior spinal surgery
- › SCS-related records (where applicable) — Pre-implant psychological evaluation report, trial stimulation documentation with contemporaneous pain scores, permanent implant records, and post-implant programming and follow-up notes
- › Functional documentation — Functional capacity evaluation reports, treating physician functional assessments, and any disability or impairment ratings relevant to vocational and functional limitation claims
- › Deposition testimony — Testimony of the treating pain management physician, the spine surgeon, any prior experts, and claimant testimony addressing symptom history, functional limitations, and the impact of the chronic pain syndrome on daily activities
Contact Expert Medical Services LLC with a brief case summary, a description of available records, and the specific pain management questions to be addressed. Engagements can be structured to address causation, standard of care, and future medical care separately or together within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Post-Laminectomy Syndrome
Post-surgical spinal pain that may follow decompression surgery for CES — causation, SCS, and future care.
CRPS Expert Witness
CRPS may develop following CES or post-decompression nerve root injury — Budapest Criteria and future care.
Spinal Cord Stimulation
SCS for refractory neuropathic pain following CES — medical necessity, cost projections, and expert testimony.
Peripheral Nerve Injury
Cauda equina nerve root injury — classification, electrodiagnostics, and neuropathic pain management.
Future Medical Care Review
Long-term pain management cost projections for CES neuropathic sequelae and neuromodulation.
Causation Analysis
Linking the traumatic or compressive event to post-CES chronic pain sequelae.
Independent Medical Evaluation
Structured IME to evaluate post-CES neuropathic pain, functional status, and treatment needs.
Expert Witness — California
Full-scope expert testimony in California CES litigation on pain management dimensions.
Arizona Pain Management Expert Witness
Cauda equina syndrome expert review for Arizona personal injury and malpractice litigation.
Medical Necessity Review
Medical necessity review for cauda equina syndrome pain management, neuromodulation, and long-term care planning.
Standard of Care Analysis
Standard of care analysis for cauda equina syndrome pain treatment and neurological complication management.
FAQ
Cauda Equina Syndrome — Common Attorney Questions
- A substantial proportion of cauda equina syndrome patients experience persistent chronic pain following surgical decompression. The most common pain patterns include bilateral radicular lower extremity pain in the distribution of the compressed nerve roots — burning, shooting, or electric quality pain in the legs, feet, or perineal region — and perineal or perianal neuropathic pain that reflects injury to the sacral nerve roots responsible for sensation in the saddle distribution. Lower back pain from the underlying disc pathology, post-surgical scarring, and secondary spinal changes is also common. Bladder and bowel dysfunction may produce associated pelvic and abdominal pain in some patients. The character and severity of post-decompression pain is highly variable — some patients experience near-complete pain resolution, while others develop a chronic neuropathic pain syndrome that requires ongoing, long-term pain management. The chronic pain sequelae of CES are distinct from the neurological deficits (motor weakness, urinary and bowel dysfunction) and require pain management specialist evaluation.
- Yes. Surgical decompression addresses the mechanical compression of the cauda equina nerve roots, but it does not reverse the neurobiological changes that have occurred in the nerve roots and the central nervous system as a result of compression. When nerve root compression has been sustained for a sufficient duration or severity, neuropathic changes — including demyelination, axon injury, and central sensitization — may persist or progress despite technically successful decompression. Central sensitization in particular — a state of amplified and persistent pain processing driven by neuroplastic changes in the spinal cord and brain — can perpetuate pain independent of ongoing structural compression. The clinical picture of post-decompression neuropathic pain in CES reflects these persistent neurobiological consequences, and the goal of chronic pain management is to reduce the pain burden and improve function rather than to eliminate the underlying structural pathology, which the surgery has already addressed.
- Spinal cord stimulation is considered for cauda equina syndrome patients with persistent refractory neuropathic pain that has not responded to an adequate course of conservative and conventional pain management. The neuropathic pain following CES — bilateral radicular lower extremity pain, perineal and perianal pain — may be amenable to SCS when it has a dermatomal or nerve root distribution that can be covered by spinal lead placement. SCS is most clearly supported when the dominant pain is neuropathic and lower extremity in distribution, the patient has failed appropriate pharmacological and interventional management, the psychological pre-implant screening evaluation is completed with favorable results, and a successful trial stimulation demonstrates meaningful pain relief. The evidence base for SCS in post-CES neuropathic pain is in part supported by the broader evidence for SCS in cauda equina and post-laminectomy neuropathic pain patterns. In personal injury litigation, future SCS costs — including trial stimulation, permanent implantation, battery replacement, and programming — may constitute a significant component of future care projections for CES patients with refractory neuropathic pain.
- Future pain management needs following CES depend on the clinical severity of the initial injury, the degree of neurological recovery after surgical decompression, and the character of the post-decompression pain syndrome. Patients with persistent neuropathic pain may require ongoing pharmacological management with neuropathic agents — gabapentinoids, SNRIs, tricyclic antidepressants — with periodic clinical reassessment and medication adjustment. Epidural steroid injections or other targeted interventional procedures may be appropriate for post-surgical radicular pain components when the pain pattern is consistent with the indication. Physical and occupational therapy for functional rehabilitation and pelvic floor rehabilitation for bladder and bowel dysfunction are recognized components of long-term CES care. In patients with refractory neuropathic pain, spinal cord stimulation may be a future care element. A complete future care projection accounts for the clinical trajectory documented in the treating record, not a generic template for all CES patients. The cost of CES-related pain management over the patient's lifetime can be substantial, particularly when advanced neuromodulation is included.
- Causation review from a pain management perspective addresses the relationship between the event that produced the cauda equina compression and the chronic pain sequelae documented in the post-surgical clinical course. This is distinct from the neurosurgical causation analysis — which addresses whether the acute CES was caused by the subject event — and from the surgical standard of care analysis, which addresses the timing and adequacy of the decompression. The pain management causation analysis considers: the temporal relationship between the cauda equina compression and the onset of chronic pain symptoms; the anatomical consistency of the pain pattern with the nerve roots that were compressed; the post-surgical imaging documentation of decompression adequacy and any persistent structural changes; the treating pain management record documenting the character, distribution, and severity of the post-decompression pain; and whether pre-existing spinal conditions, prior episodes of back or leg pain, or prior surgical interventions could contribute to the current pain presentation. Opinions are case-specific and are grounded in the available records.
- Cauda equina syndrome is classified as complete (CESC) or incomplete (CESI) primarily based on bladder function at presentation. In incomplete CES (CESI), the patient experiences urinary symptoms — difficulty with initiation, incomplete emptying, altered sensation — but retains some degree of voluntary bladder control. In complete CES (CESC), the patient presents with painless urinary retention — complete loss of bladder sensation and voluntary control. The distinction is prognostically significant: patients presenting with CESI generally have better neurological recovery than those presenting with CESC. In the litigation context, the CESI/CESC classification affects future care projections in two ways. First, the neurological recovery trajectory and the expected residual deficit differ between the two presentations — CESC is associated with higher rates of permanent bladder dysfunction and more severe persistent neurological deficits. Second, the chronic pain trajectory differs — CESC is generally associated with more severe and persistent post-decompression neuropathic pain that requires more intensive long-term pain management. The completeness classification should be documented in the treating record from initial presentation, and its absence may be a medical documentation deficiency in a case where prognosis and future care are contested.
- The pain management standard of care for post-decompression CES patients reflects the obligations of a reasonably competent pain management physician assuming care of a patient with persistent neuropathic pain following surgical cauda equina decompression. Core elements include: an initial evaluation that characterizes the specific pain generators present and correlates them with the documented nerve root injury pattern; a treatment approach that is matched to the neuropathic character of post-CES pain rather than primarily axial or mechanical; an adequate trial of first-line neuropathic agents before escalation to interventional procedures; recognition and documentation of the bowel and bladder dysfunction dimensions of the pain syndrome; appropriate monitoring and documentation of any opioid prescribing; and timely consideration of referral to neuromodulation when the pain is refractory to conservative management. This expert opinion scope is limited to pain management standard of care — the timing of surgical decompression, the adequacy of surgical technique, and the neurosurgical standard of care are outside this scope and require a spine surgery or neurosurgery expert.
- Even following complete surgical decompression, cauda equina syndrome produces functional limitations that may persist long-term and significantly affect quality of life, activities of daily living, and vocational capacity. Urinary dysfunction — including reduced bladder sensation, incomplete bladder emptying, urinary urgency, or residual urinary incontinence — is common and may require ongoing urological management and assistive strategies. Bowel dysfunction — including reduced rectal sensation, altered defecation urgency, or fecal incontinence — affects daily functioning and social participation. Sexual dysfunction is documented in the CES literature as a frequent long-term sequela. Persistent bilateral lower extremity weakness, altered gait, and reduced ambulatory capacity may limit standing and walking tolerance. Chronic neuropathic pain — particularly perianal and perineal pain from sacral nerve root injury — affects sitting tolerance and activities requiring sustained positioning. These functional limitations are the combined consequence of neurological injury (motor and sensory deficit) and the chronic pain syndrome, and both dimensions require independent expert evaluation: the neurological deficits require a neurologist or physiatrist expert, and the chronic pain sequelae require a pain management expert.
- Key records for a complete pain management expert review in a CES case include: initial emergency or urgent care records documenting the acute presentation — onset and character of symptoms, neurological examination findings including saddle sensation testing and bladder function assessment; imaging studies from the acute presentation — MRI of the lumbar spine identifying the level and degree of compression; operative reports from the decompression surgery documenting the surgical findings, the degree of compression encountered, the procedure performed, and the post-decompression spinal examination findings; post-surgical imaging documenting the adequacy of decompression; the complete treating pain management records from the initial post-surgical pain management evaluation through the most recent encounter; physical and occupational therapy records from the rehabilitation period; urological records if bladder dysfunction has been separately evaluated and treated; prior lumbar spine records to establish baseline and document any pre-existing disc disease; and any prior independent medical examination or expert opinion reports. Where future care is at issue, the current treating physician's assessment of long-term prognosis and future treatment recommendations is an important additional record.
- Yes. Dr. Dardashti accepts cauda equina syndrome engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides — on the pain management dimensions of the case. This includes causation of chronic neuropathic pain sequelae, standard of care review for post-decompression pain management, medical necessity of treatment rendered, and future medical care projections. Expert review is limited to pain management and anesthesiology — surgical timing, neurosurgical technique, and the standard of care for emergency decompression are outside this scope and require a spine surgery or neurosurgery expert. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain Dr. Dardashti for a Cauda Equina Syndrome Case
Dr. Dardashti accepts CES engagements for both retaining parties on the pain management dimensions of CES litigation. Contact Expert Medical Services LLC to discuss case scope and availability.