Nationwide Pain & Injury Medical Expert Witness
Radiofrequency Ablation Expert Witness: Medical Necessity, Standard of Care, and Litigation Review
Independent expert review of radiofrequency ablation procedures, diagnostic requirements, patient selection, technical execution, complications, causation, and future medical care issues in personal injury and medical malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Topic
- Radiofrequency Ablation (RFA)
- Also Known As
- Radiofrequency Neurotomy, Facet Rhizotomy, Medial Branch RFA
- Specialty
- Interventional Pain Management
- Evaluation Areas
- Medical Necessity, Standard of Care, Causation, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Radiofrequency Ablation in Litigation
Radiofrequency ablation is among the most frequently performed and most frequently disputed interventional pain procedures in personal injury and medical malpractice litigation. Its position at the end of a required diagnostic sequence makes the adequacy of the preceding workup a threshold issue in nearly every RFA dispute. Its recurring nature — driven by medial branch nerve regeneration — makes future RFA a standard element of damages analysis in cases involving facet-mediated spinal pain.
RFA litigation raises a defined set of questions that require a pain management specialist to address: Was the diagnostic pathway properly followed? Were the medial branch blocks that preceded it adequately documented? Was the procedure performed at the correct levels with the correct technique? Were complications the result of a deviation from the standard of care? What does a defensible future care projection for a patient requiring serial RFA look like? These are pain management questions — not surgical questions — and they require a board-certified pain management physician to answer them.
What Is Radiofrequency Ablation?
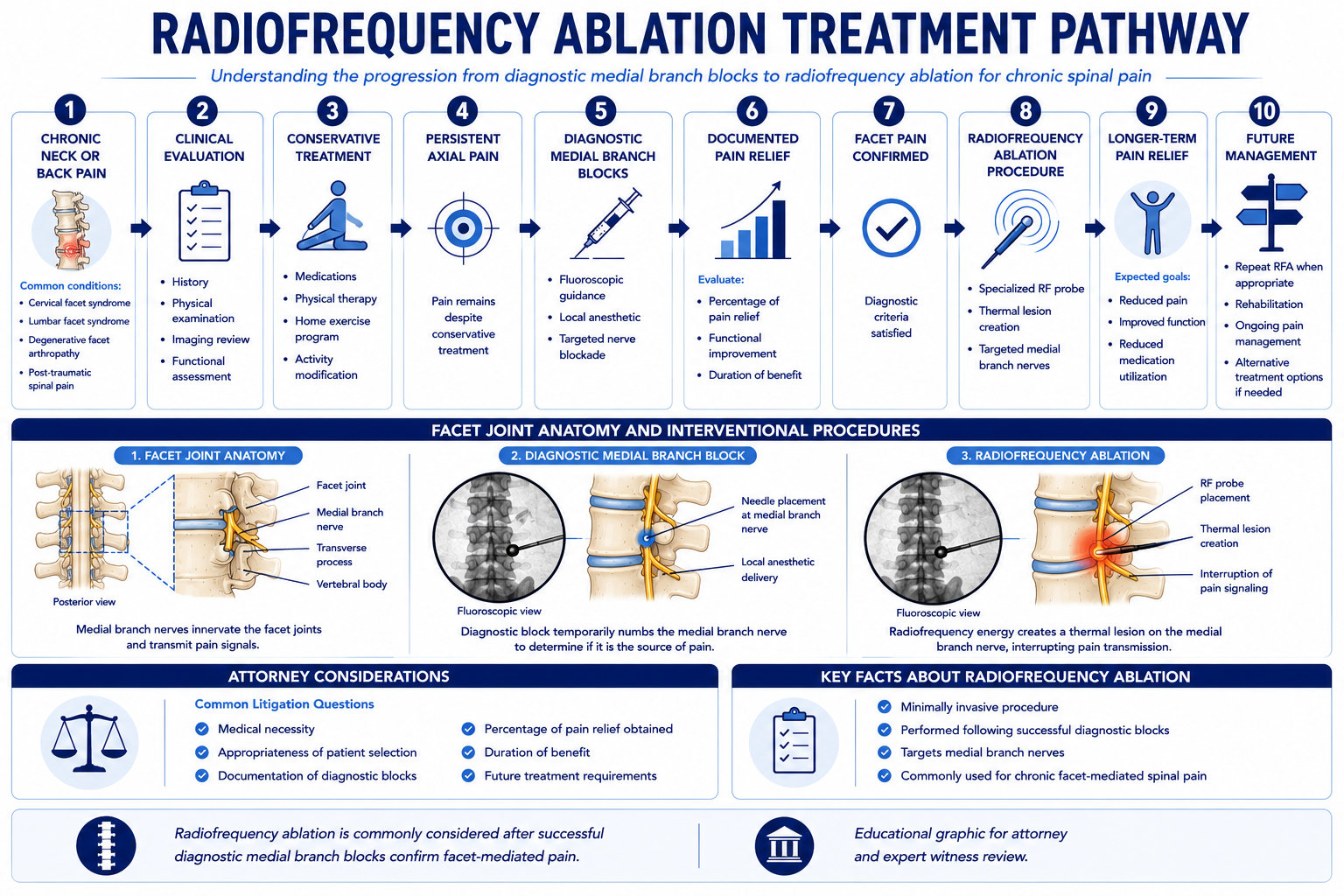
Radiofrequency ablation — also called radiofrequency neurotomy or facet rhizotomy — is an interventional pain procedure that uses radiofrequency energy delivered through a specialized needle to create a controlled thermal lesion on the medial branch nerves supplying the cervical or lumbar facet joints. By heating the nerve to a temperature that disrupts its ability to transmit pain signals, RFA produces relief of facet-mediated axial spinal pain that outlasts a local anesthetic block by months rather than hours.
Facet joints — the paired zygapophyseal joints at each vertebral level — receive sensory innervation from the medial branch nerves, small rami of the posterior primary divisions of the spinal nerve roots. Because each facet joint is innervated by medial branches from two consecutive spinal levels, RFA requires treatment of medial branches at two levels to fully denervate a single joint. In the lumbar spine, the L5 dorsal ramus (not a medial branch) supplies the L5–S1 facet joint and is the target at that level. The distinction between these anatomical targets is relevant to both the technical standard of care and the documentation required to support the procedure.
The thermal lesion is created by placing the radiofrequency needle with its active tip parallel and in close proximity to the target nerve — a precise positioning requirement that distinguishes RFA from other interventional procedures and makes fluoroscopic guidance and technique adherence essential elements of the standard of care. Sensory and motor testing before the lesion is generated allows confirmation of appropriate electrode placement and reduces the risk of unintended adjacent structure involvement.
The expected duration of benefit from a single RFA procedure is typically six to twelve months — limited by the biological process of medial branch nerve regeneration. When the nerve regenerates, the patient may again experience facet-mediated pain at the treated levels, and repeat ablation may be indicated if the clinical pattern is consistent and the original procedure produced adequate documented relief. This predictable regeneration timeline is what makes serial RFA a recognized long-term treatment strategy and a standard element of future medical care projections in personal injury damages analysis.
The Diagnostic Pathway Before Radiofrequency Ablation
The confirmatory medial branch block protocol is the clinical and regulatory gateway to radiofrequency ablation. Because RFA creates a semi-permanent disruption of nerve function, clinical guidelines and most payer policies require that the facet joint be identified as the pain generator through a defined diagnostic sequence before ablation is authorized. The core requirement — two separate positive medial branch blocks at the intended levels — is both a standard of care expectation and a medical necessity threshold.
A positive response to a medial branch block is defined as a specified percentage reduction in targeted axial pain lasting for the expected duration of the local anesthetic used. Most clinical guidelines require at least 50% improvement; some payer criteria require 80%. Short-acting agents such as lidocaine are expected to produce relief for one to four hours; longer-acting agents such as bupivacaine for four to eight hours or more. To reduce placebo response, some protocols require that the two confirmatory blocks use different local anesthetic agents — and the duration of relief documented after each block should correlate to the pharmacokinetic profile of the agent used at that block.
Documentation of each confirmatory block is critical to the medico-legal record. The procedure report should specify: the targeted levels; the local anesthetic agent and volume used; and the patient-reported percentage of pain improvement at defined time intervals post-procedure. This documentation must be contemporaneous — recorded at or immediately following the procedure encounter — to be clinically credible and legally defensible. Retrospective documentation of relief percentages or duration, or documentation that is identical across multiple block encounters regardless of the agent used, raises substantial credibility and standard of care concerns.
- › Single block vs. dual confirmatory blocks — Some older protocols accepted a single positive medial branch block as sufficient to proceed to RFA. Current clinical guidelines from the American Society of Interventional Pain Physicians (ASIPP) and the International Spine Intervention Society (ISIS) recommend two separate confirmatory blocks. Cases involving RFA preceded by only one block may involve a necessity dispute that turns on which guidelines were applicable at the time of treatment.
- › Relief percentage threshold — Whether 50% or 80% relief is the applicable threshold depends on the guidelines and payer criteria in effect at the time of treatment. The treating physician's documentation should reflect awareness of the applicable standard and record relief against the threshold criterion used.
- › Level concordance — The levels treated with RFA should correspond to the levels at which confirmatory blocks produced positive responses. Treating additional or different levels at the time of RFA — without confirmatory blocks at those levels — is a frequent subject of both standard of care and necessity review.
- › Common documentation failures — Missing post-procedure pain assessments; identical relief percentages across multiple blocks regardless of agent used; no record of the anesthetic agent or volume; absence of fluoroscopy documentation; and level discrepancies between blocks and subsequent RFA are the most frequent documentation deficiencies arising in medical necessity and standard of care reviews.
Medical Necessity Considerations
Medical necessity for radiofrequency ablation is evaluated against the clinical record and applicable treatment guidelines. A supported indication generally requires: documented chronic axial spinal pain consistent with facet-mediated origin; failure of conservative management to provide adequate relief; a clinical examination consistent with facet joint involvement at the proposed levels; relevant imaging findings; and a documented positive response to two confirmatory medial branch blocks at those levels. The confirmatory block protocol is not merely a payer requirement — it is the clinical mechanism by which the target pain generator is identified before ablation.
Chronicity and conservative care failure are threshold elements of the necessity analysis. Facet-mediated pain from an acute injury may resolve with conservative treatment, and interventional procedures performed very early in the post-injury course — before an adequate conservative trial — may face necessity scrutiny. Conversely, persistent axial pain that has been documented over an appropriate period, has not responded to physical therapy and analgesic management, and has a pattern consistent with facet-mediated origin generally supports necessity for the diagnostic evaluation leading to RFA. The adequacy of the conservative treatment record is a threshold issue in most insurance necessity reviews. For the full clinical evaluation framework that underlies a pain management physician's assessment of axial pain — including examination findings, functional assessment, and validated instruments — see the article on how pain management experts objectively evaluate pain.
Pre-existing degenerative changes at the facet levels do not preclude medical necessity for RFA related to a new injury or aggravation. Facet arthrosis and joint hypertrophy are common degenerative findings in the general population. Their presence does not establish that the treatment was unrelated to the claimed injury — rather, it requires careful analysis of the pre-accident baseline and the clinical changes documented after the event. Causation analysis addresses the distinction between pre-existing facet degeneration and facet-mediated pain causally related to the subject incident.
Repeat RFA necessity is evaluated against documented prior benefit. When initial ablation produced adequate and documented relief and the patient returns with recurrence of the same axial pain pattern at the treated levels within the expected regeneration timeline, repeat ablation at the same levels is clinically supported. Repeat procedures without documentation of prior benefit, at frequencies inconsistent with nerve regeneration timelines, or at levels different from those previously confirmed and treated, raise necessity concerns that are commonly raised in insurance disputes and defense review.
Standard of Care Considerations
The standard of care for radiofrequency ablation reflects the practice of a reasonably competent board-certified or board-eligible pain management physician performing the procedure in accordance with current professional guidelines. Core elements include appropriate patient selection through a complete diagnostic evaluation, adherence to the confirmatory block protocol, use of fluoroscopic guidance with defined electrode placement technique, pre-lesion sensory and motor testing, and contemporaneous documentation of the procedure and patient response.
- › Fluoroscopic guidance — RFA requires fluoroscopic guidance to confirm electrode placement in the appropriate anatomical position relative to the target medial branch nerve. Procedures performed without fluoroscopy cannot reliably achieve the electrode alignment necessary for effective lesioning and are below the standard of care.
- › Parallel electrode placement — Effective thermal lesioning requires that the active tip of the RFA needle be positioned parallel and in close proximity to the target nerve. Perpendicular placement produces a smaller, less reliable lesion and is a recognized technical deviation associated with treatment failure. Documentation of fluoroscopic needle position is relevant to standard of care review in cases involving inadequate relief or nerve injury.
- › Sensory testing — Pre-lesion sensory stimulation at 50 Hz is used to confirm proximity of the electrode to the target nerve by reproducing the patient's concordant pain at low voltage thresholds. This step confirms appropriate positioning before the thermal lesion is created and is a standard element of the RFA procedure record.
- › Motor testing — Pre-lesion motor stimulation at 2 Hz at higher voltage thresholds tests for proximity of the electrode to the adjacent exiting nerve root, which carries motor fibers. Absence of motor response at appropriate thresholds before lesioning is the standard precaution against unintended motor nerve injury. Documentation of motor testing parameters and results is reviewed in nerve injury claims.
- › Lesion parameters — Standard lumbar medial branch RFA is typically performed at 80–90°C for 60–90 seconds per lesion site. Cervical RFA parameters vary by protocol. Deviation from recognized lesion parameters — either below thresholds that may fail to achieve adequate denervation, or above thresholds that may injure adjacent structures — is relevant to standard of care review in outcome-based claims.
- › Local anesthetic before lesioning — Administration of local anesthetic at the RFA electrode tip before thermal lesion generation reduces post-procedure neuritis. Its omission in cases where significant post-procedure pain occurred may be relevant to standard of care review.
- › Confirmatory block adherence — Proceeding to RFA without two documented positive confirmatory medial branch blocks at the intended levels is a deviation from standard clinical practice. The adequacy of the preceding diagnostic workup is a threshold standard of care issue in every RFA malpractice case.
Common Litigation Issues
Radiofrequency ablation cases present a defined pattern of litigation issues across personal injury and medical malpractice contexts. The most significant issues cluster around the adequacy of the preceding diagnostic workup, the technical execution of the procedure, and the clinical basis for repeat ablation.
- › Inadequate diagnostic confirmation before RFA — Proceeding to ablation without two documented positive confirmatory blocks — or with blocks whose documentation does not demonstrate the required relief percentage and duration — is the most common medical necessity and standard of care dispute in RFA litigation. This issue arises in both malpractice claims (where the inadequacy of the workup is the alleged deviation) and insurance disputes (where the payer denies necessity based on documentation failure).
- › Wrong-level treatment — RFA at levels not supported by positive confirmatory blocks, or at anatomically incorrect positions based on fluoroscopy review, is a recognized malpractice basis. Wrong-level treatment may result in treatment failure, ongoing pain, and potential injury to untargeted structures. Fluoroscopy records and procedure documentation are reviewed to evaluate the accuracy of electrode placement.
- › Inappropriate patient selection — RFA performed in patients with radicular pain patterns rather than axial facet-mediated pain, with alternative pain generators not excluded, or in the absence of an adequate conservative treatment trial, raises both necessity and standard of care questions. Misidentification of the pain source before ablation is a root cause of treatment failure claims.
- › Repeat RFA disputes — Defense counsel and insurers commonly dispute the necessity of repeat ablation procedures, challenging whether prior RFA produced documented benefit sufficient to justify retreatment, whether the interval between procedures is consistent with nerve regeneration timelines, and whether the same levels remain the appropriate target.
- › Billing disputes — RFA is billed per level treated. Treatment of multiple levels generates substantially higher reimbursement. Disputes arise when the number of levels billed is not supported by clinical documentation, when levels billed differ from levels described in the procedure report, or when billing reflects RFA at levels for which no confirmatory blocks were performed.
- › Causation disputes — Whether the facet-mediated pain requiring RFA arose from the subject accident, aggravated a pre-existing condition, or was unrelated to the claimed injury is a central question in personal injury matters involving RFA treatment or proposed future RFA as damages.
- › Post-procedure complications attributed to technique — Neuritis, dysesthesia, and sensory changes following RFA may be the subject of malpractice claims where the plaintiff contends the complication resulted from a technical deviation. Expert review of the procedure report, fluoroscopy records, and stimulation parameters is required to evaluate whether the complication was a recognized risk of the procedure or a consequence of substandard technique.
Personal Injury Case Analysis
Motor vehicle collisions are the most common mechanism of traumatic facet joint injury in the personal injury context. Rear-impact collisions generate a hyperextension-flexion mechanism that places significant mechanical stress on the cervical facet joints and capsular ligaments — cervical facet pain is one of the most well-documented persistent pain syndromes following whiplash-mechanism injuries. Biomechanical and post-mortem imaging research has demonstrated capsular tears and hemorrhagic changes in facet joints following rear-impact collisions at speeds producing minimal vehicle damage, supporting a causal mechanism even in low-energy impacts. Lumbar facet injuries may follow axial loading, rotational forces, or direct impact.
In personal injury matters where RFA has been performed or is proposed as future care, causation review addresses several questions distinct from whether the procedure was clinically appropriate. These include: whether the accident produced or aggravated facet-mediated pain at the treated levels; whether pre-existing facet degeneration documented on imaging was symptomatic or asymptomatic before the accident; whether the temporal relationship between the accident and the onset of documented axial pain is consistent with a traumatic mechanism; and whether the clinical course supports a continuous and causal relationship between the event and the need for interventional treatment.
Apportionment is a recurring issue in cases involving significant pre-existing facet degeneration. The presence of facet arthrosis does not establish that the accident was not a contributing cause of the pain requiring treatment. A person with pre-existing degenerative facet disease who sustains a traumatic capsular injury can require interventional treatment — including the full MBB-to-RFA diagnostic and treatment pathway — that the same person would not have required absent the accident. Expert causation analysis addresses the distinction between the natural history of pre-existing degeneration and the acceleration or aggravation produced by the subject event.
When facet-mediated pain persists despite adequate RFA and does not respond to repeat ablation, further escalation — including consideration of spinal cord stimulation for refractory axial pain — may become a future care component in high-value personal injury matters. The trajectory from conservative treatment through confirmatory blocks, initial RFA, repeat ablation cycles, and potential escalation to neuromodulation is a treatment pathway that expert review can address comprehensively within a single retention for future medical care projection purposes.
Medical Malpractice Analysis
Malpractice claims involving radiofrequency ablation generally arise from inadequate diagnostic workup before the procedure, technical errors in electrode placement or lesioning, complications attributed to technique deviations, or treatment at incorrect levels. Expert review addresses whether the care provided by the treating pain management physician met the applicable standard of care for a board-certified specialist performing RFA in the relevant clinical context.
- › Failure to complete the required diagnostic block protocol — Performing RFA without two documented positive confirmatory medial branch blocks at the targeted levels is a recognized departure from the clinical standard. This is the most common standard of care issue raised in RFA malpractice claims and is typically addressed through review of the procedure records preceding the ablation.
- › Wrong-level or wrong-site ablation — Thermal lesioning at levels not confirmed by prior blocks, or at anatomically incorrect positions due to targeting error, may result in treatment failure and potential injury to untargeted structures. Fluoroscopy records and procedure documentation are reviewed to evaluate the accuracy of electrode placement at the time of the procedure.
- › Nerve root or dorsal root ganglion injury — RFA electrode placement that is too medial or too deep can result in injury to the exiting nerve root or dorsal root ganglion, producing radicular pain, sensory loss, or motor deficit. Pre-lesion motor testing at 2 Hz is the standard precaution against this complication. Claims addressing nerve root injury require review of the stimulation testing documentation and the fluoroscopic needle position at the time of lesioning.
- › Post-procedure neuritis vs. technical complication — A transient post-RFA neuritis — characterized by increased pain at the treated levels for two to six weeks — is a recognized expected sequela of successful RFA and should be distinguished from prolonged or worsening pain indicating a technical complication. Failure to counsel the patient about expected post-procedure neuritis may raise informed consent issues in cases where the patient presents emergently or returns for pain unrelated to a true complication.
- › Failure to identify an alternative pain generator — When RFA fails to produce the expected relief despite technically adequate performance and proper confirmatory block documentation, the treating physician's obligation includes reconsidering whether the facet joint is the primary pain generator or whether an alternative source — disc pathology, radiculopathy, sacroiliac joint dysfunction, or a competing diagnosis — was overlooked. Failure to reconsider the diagnostic basis for treatment in the setting of a failed ablation may be relevant to standard of care review.
- › Informed consent — The standard of care requires that informed consent address the purpose of the procedure, recognized risks (including neuritis, nerve injury, infection, and treatment failure), the expected duration of benefit, the nerve regeneration timeline and its implications for repeat procedures, and the alternatives. Failure to adequately address the temporary nature of RFA relief is relevant where the patient later objects that they were not informed the procedure would require serial repetition.
Expert review is within the scope of pain management and anesthesiology. Opinions on neurosurgical or spine surgical technique are outside this scope. The retaining attorney should identify the specific standard of care questions to be addressed at the time of engagement initiation.
Future Medical Care Review
Future radiofrequency ablation is one of the most common interventional pain components in future medical care projections for personal injury cases involving facet-mediated spinal pain. Because medial branch nerves regenerate over time — typically within six to twelve months — a patient with documented facet-mediated pain who responded to initial RFA will predictably require repeat ablation at regular intervals for the duration of the condition. This recurrent treatment structure means that the aggregate future cost of RFA can be substantial in high-value cases, and the defensibility of that projection depends on the quality of the underlying medical record.
A defensible future RFA projection requires: a medical record documenting the original diagnosis and the diagnostic block sequence; documented benefit from prior RFA; a clinical basis for expecting the facet-mediated pain to persist; a treatment frequency consistent with the nerve regeneration timeline; an itemized cost structure accounting for the procedure, facility, and anesthesia costs at each cycle; and a defined duration of need grounded in clinical prognosis rather than an assumed lifetime projection without clinical support.
- › Repeat cycle frequency — The expected interval between repeat RFA procedures is typically six to twelve months and is grounded in the known timeline of medial branch nerve regeneration. Projected frequencies inconsistent with this timeline require clinical justification and are subject to challenge in future care disputes.
- › Confirmatory block costs per cycle — Future medical care projections should account for the medial branch blocks required before each repeat RFA cycle. Because the nerve regeneration pattern is predictable and re-confirmation of appropriate level selection before repeat ablation is clinically appropriate, future confirmatory blocks are a recognized per-cycle component of the treatment cost structure.
- › Escalation to neuromodulation — When facet-mediated axial pain becomes refractory to serial RFA — through waning response, changing pain generators, or concurrent central sensitization — escalation to spinal cord stimulation may be a clinically supported future care option where the medical record supports this trajectory. The basis for projecting this escalation, and the cost structure associated with SCS, is addressed as part of a comprehensive future care review.
- › Geographic cost variation — Facility, physician, and anesthesia costs for RFA vary materially by geographic market. Future care projections should reflect costs in the plaintiff's treating market and distinguish between outpatient surgery center and hospital-based procedure costs where the distinction affects the aggregate projection.
Future medical care review for RFA cases can be structured as a standalone engagement or combined with causation analysis in cases where both are at issue. Contact Expert Medical Services LLC to discuss the scope and available records.
Expert Witness Review Process
Radiofrequency ablation cases require review of a defined set of records to support a complete medical-legal opinion. The scope of records needed depends on whether the engagement addresses medical necessity, standard of care, causation, future care, or a combination of these issues. Typical records include:
- › Complete treating pain management records — Initial evaluation, follow-up clinical notes, pre-procedure assessments, and post-procedure response documentation for each medial branch block and RFA encounter, from the beginning of the pain management relationship through the most recent visit
- › Procedure reports and fluoroscopy documentation — Procedure reports for each medial branch block and RFA session; fluoroscopy images or records documenting needle and electrode placement; contrast confirmation for blocks; and stimulation testing documentation for RFA (sensory and motor testing parameters and responses)
- › Post-block pain assessment records — Contemporaneous documentation of the percentage and duration of pain relief following each confirmatory medial branch block — the evidentiary foundation for RFA authorization and the primary document reviewed in medical necessity analysis
- › Pre-procedure spinal imaging — MRI or CT of the relevant spinal segment(s), to evaluate the degree and pattern of facet degeneration, the presence of disc pathology or nerve compression, and structural findings at the proposed treatment levels
- › Billing records — Itemized billing by CPT code and date of service, to evaluate consistency between procedures billed and procedures documented in the clinical and procedure records; essential in billing dispute and unnecessary treatment claims
- › Insurance authorization records — Pre-authorization requests, payer criteria applied, and denial or approval documentation in cases where a medical necessity dispute with a payer is at issue
- › Prior treating physician records — Records from treating physicians predating the pain management relationship, to establish the pre-injury or pre-procedure baseline, prior treatment history, and absence or presence of pre-existing symptoms at the involved levels
- › Deposition testimony — Testimony of the treating pain management physician addressing clinical rationale, patient-reported response, procedural decisions, and the basis for level selection — as well as claimant testimony and testimony of any retained experts addressing overlapping issues
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. Engagements addressing medical necessity, standard of care, causation, and future medical care can be structured separately or together within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Medial Branch Block
Expert review of MBB medical necessity, standard of care, and the diagnostic pathway required before radiofrequency ablation.
Epidural Steroid Injections
Expert evaluation of ESI medical necessity, standard of care, causation, and future care — the radicular treatment pathway distinct from facet-mediated RFA.
CRPS Expert Witness
Complex Regional Pain Syndrome — diagnosis, causation, Budapest Criteria, and future care review.
Spinal Cord Stimulation
Neuromodulation for refractory pain — medical necessity, cost projections, and expert testimony.
Post-Laminectomy Syndrome
Persistent spinal pain following surgery — causation, treatment appropriateness, and future care.
Peripheral Nerve Injury
Expert evaluation of nerve injury, electrodiagnostic findings, and neuropathic pain in complex litigation.
Future Medical Care Review
Projecting repeat RFA cycles, frequency, and long-term pain management costs for damages analysis.
Causation Analysis
Linking the mechanism of trauma to facet joint injury and the need for radiofrequency ablation.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California RFA matters.
Arizona Pain Management Expert Witness
Radiofrequency ablation expert review for Arizona personal injury and malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for radiofrequency ablation — diagnostic block adequacy, procedural justification, and repeat procedure review.
Standard of Care Analysis
Standard of care analysis for radiofrequency ablation technique, patient selection, and outcome documentation.
FAQ
Radiofrequency Ablation — Common Attorney Questions
- Radiofrequency ablation (RFA) is a fluoroscopically guided pain management procedure that uses radiofrequency energy to create a controlled thermal lesion on the medial branch nerves supplying the cervical or lumbar facet joints. By interrupting the nerve's ability to transmit pain signals from the facet joint, RFA produces longer-duration relief than a diagnostic medial branch block. The effect is semi-permanent — the targeted nerves eventually regenerate, typically within six to twelve months — making repeat procedures a recognized component of long-term facet pain management.
- Yes. Clinical guidelines and most payer policies require that at least two separate positive medial branch blocks precede radiofrequency ablation at the same levels. This requirement exists because RFA creates a more definitive, longer-lasting effect than a diagnostic block, and the confirmatory protocol verifies that the targeted facet levels are the actual pain generators before an ablative procedure is performed. Proceeding to RFA without adequate confirmatory blocks is a recognized standard of care deviation and a frequent basis for medical necessity disputes.
- The treating physician's records should document: two separate medial branch blocks at the intended levels; the local anesthetic agent and volume used at each block; the patient-reported percentage of pain improvement following each block (typically at least 50%, with some guidelines requiring 80%); the duration of relief (which should correlate to the pharmacokinetic profile of the agent used); and the clinical basis for selecting the specific levels to be treated. Procedure reports and fluoroscopy records documenting needle placement and contrast confirmation should accompany each block. Absence of this contemporaneous documentation is one of the most common medical necessity and standard of care issues in RFA litigation.
- Most clinical guidelines define a positive response as at least 50% reduction in targeted axial pain, lasting for the expected duration of the local anesthetic used. Some payer criteria and clinical protocols require 80% relief. Short-acting agents such as lidocaine are expected to produce relief lasting one to four hours; longer-acting agents such as bupivacaine for four to eight hours or more. To reduce the possibility of placebo response, some protocols require that the two confirmatory blocks use different local anesthetic agents — and the duration of relief documented after each block should correlate to the pharmacokinetic profile of the agent used at that block.
- Causation review addresses whether the subject motor vehicle collision produced or aggravated facet-mediated pain in the cervical or lumbar spine sufficient to require interventional treatment, including RFA. Rear-impact collisions generate a hyperextension-flexion mechanism that places significant stress on the cervical facet joints, and cervical facet pain is a well-documented cause of chronic axial neck pain following whiplash-mechanism injuries. Lumbar facet injuries may follow axial loading or rotational forces. Causation analysis evaluates the temporal relationship between the accident and the onset of documented pain, the clinical consistency of the pain pattern, the mechanism of injury, and the pre-accident baseline history and imaging.
- Recognized complications of RFA reviewed in malpractice matters include: wrong-level treatment (ablation at levels not supported by confirmatory blocks); thermal injury to adjacent structures from incorrect needle placement or lesioning parameters; post-procedure neuritis (a transient flare of nerve pain that should be distinguished from a technical complication); inadvertent injury to the spinal cord, exiting nerve root, or dorsal root ganglion; infection; and failure to identify an alternative pain generator that explains ongoing pain despite technically adequate RFA. Claims also arise from inadequate diagnostic workup before the ablative procedure and from failure to obtain informed consent addressing the risks and the nerve regeneration timeline.
- Medial branch nerves regenerate over time — typically within six to twelve months — and repeat RFA procedures at the same levels are clinically recognized when the original procedure produced adequate relief and the patient returns with recurrence of the same pain pattern at the same levels. Most clinical guidelines and payer policies permit repeat RFA at intervals consistent with the known regeneration timeline, provided that prior RFA at those levels produced documented benefit. Repeat procedures without prior documented benefit, at frequencies inconsistent with nerve regeneration timelines, or at levels not previously treated with confirmatory blocks may be subject to medical necessity scrutiny.
- Yes. Future RFA is a recognized component of long-term pain management planning for patients with documented facet-mediated spinal pain who have responded to prior ablation. Future medical care projections typically account for the expected frequency of repeat RFA cycles (consistent with the nerve regeneration timeline), the cost of each procedure cycle (including associated facility and anesthesia costs), confirmatory block costs before each repeat cycle, the duration of projected future need, and the clinical basis for expecting the condition to persist. These projections are a discrete element of damages analysis in personal injury litigation and require a physician opinion grounded in the available medical record.
- Key records include: complete treating pain management notes from initial evaluation through the most recent encounter; procedure reports and fluoroscopy documentation for each medial branch block and RFA procedure performed; post-procedure pain assessment records documenting the percentage and duration of relief following each block; pre-procedure spinal imaging (MRI or CT of the relevant segment); billing records itemized by CPT code and date of service; insurance authorization records and payer correspondence; prior treating physician records predating the pain management relationship; and, where applicable, deposition testimony of the treating pain management physician addressing clinical rationale and patient-reported response.
- Yes. Dr. Dardashti accepts radiofrequency ablation engagements for both plaintiff and defense counsel, as well as insurance defense and medical malpractice matters. Review is available for the full scope of RFA-related issues — medical necessity, standard of care, causation, and future medical care — or for defined subsets of those issues based on the questions the retaining attorney needs addressed. Engagements are structured after a brief case summary is provided to confirm the scope and availability.
Retain a Radiofrequency Ablation Expert for Your Case
Dr. Dardashti accepts radiofrequency ablation engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.