Nationwide Pain & Injury Medical Expert Witness
Pain Management Standard of Care Analysis
Physician-level standard of care analysis for pain management procedures, interventional treatments, and implanted devices. Written opinion structured for deposition and trial. Plaintiff and defense.
Request AvailabilityCredentials & Qualifications
- Service
- Standard of Care Analysis & Written Opinion
- Specialty
- Pain Management & Anesthesiology
- Board Certification
- American Board of Anesthesiology
- Standards Applied
- Published Guidelines, Peer-Reviewed Evidence
- Available For
- Plaintiff & Defense
- Jurisdiction
- California — Nationwide
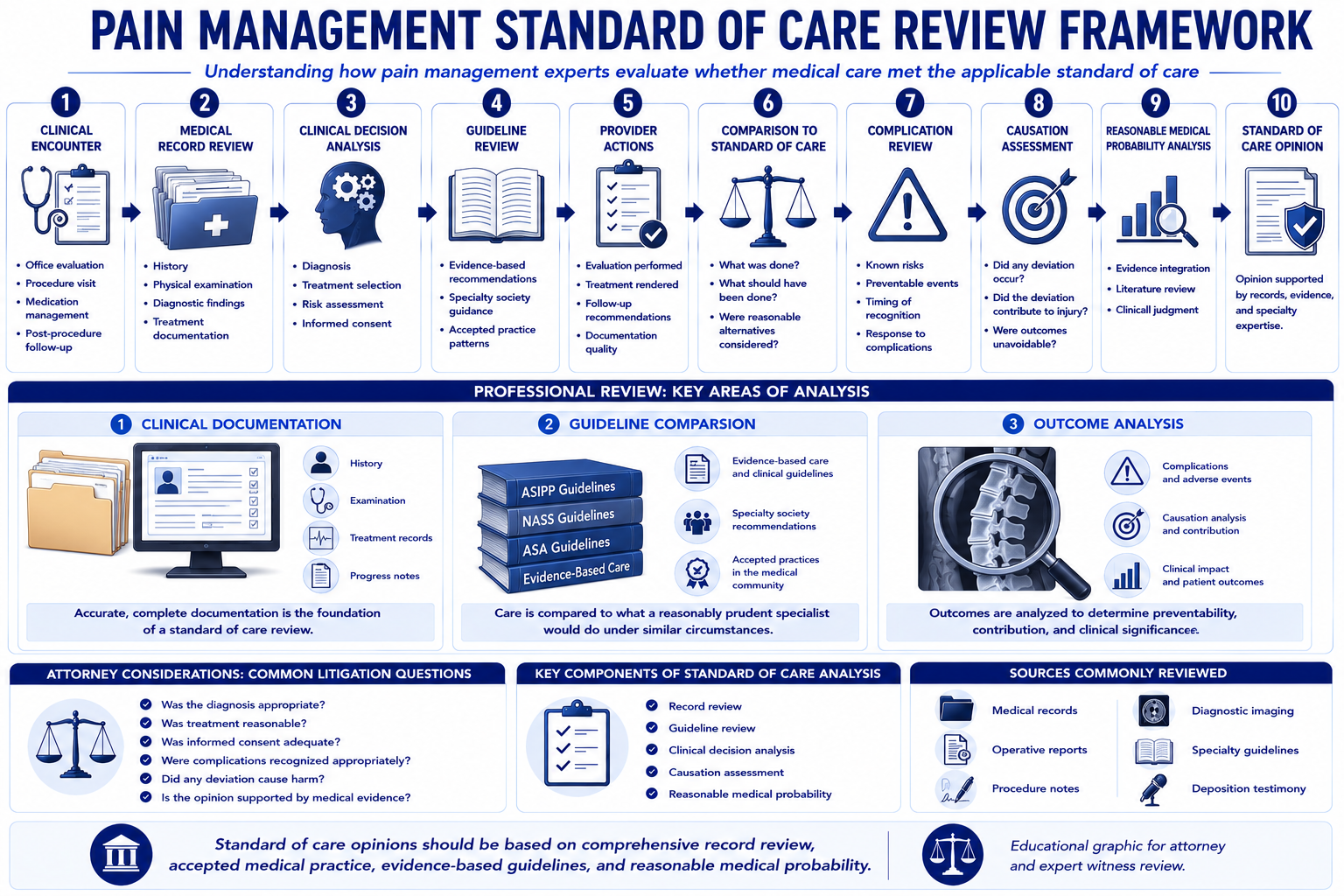
What Is Standard of Care Analysis?
A pain management standard of care analysis is a physician's structured written opinion on whether the clinical conduct of a treating pain management specialist — including diagnostic decisions, procedural selection, technique, documentation, informed consent, and follow-up — conformed to the standard of care applicable to a qualified pain management physician under similar circumstances. It is the evidentiary foundation of every medical malpractice case involving pain management, and it is a recurring issue in personal injury cases where the adequacy of treatment is contested alongside causation and damages.
The standard of care is not a single protocol or a rigid checklist. It reflects what a reasonably competent pain management specialist, exercising the knowledge and skill appropriate to the specialty, would have done in the same or similar clinical circumstances. That standard is established through published clinical guidelines, peer-reviewed literature, specialty society practice standards, and the testimony of qualified physician experts. An opinion that does not engage this body of evidence — that asserts a standard without identifying its source — will not withstand cross-examination at deposition or trial. A standard of care review that addresses documentation of objective examination findings requires an understanding of what a competent pain management physician's evaluation encompasses; for that methodology, see the article on how pain management experts objectively evaluate pain.
Dr. Dardashti provides standard of care opinions across the full scope of pain management practice: epidural injections, nerve blocks, radiofrequency ablation, neuromodulation, intrathecal drug delivery, opioid prescribing, and the full spectrum of procedures and clinical decisions made by pain management specialists. Opinions are available for plaintiff and defense counsel, insurance carriers, government agencies, mediators, and courts.
Why Standard of Care Matters in Litigation
In medical malpractice litigation, the standard of care is the central contested issue. The plaintiff must establish that the defendant's conduct deviated from the applicable standard, that the deviation caused the claimed harm, and that the harm produced compensable damages. A plaintiff who cannot establish the standard, cannot identify a departure from it, and cannot connect that departure to the harm will not prevail — regardless of how severe the outcome.
In personal injury litigation, standard of care issues arise in a different but equally important context: whether the treatment rendered by the plaintiff's pain management physicians was appropriate, within guidelines, and consistent with accepted clinical practice. Defense experts who challenge the necessity or appropriateness of treatment are implicitly making standard of care arguments — asserting that a competent pain management physician would not have pursued the treatment pathway the plaintiff's doctors chose. Plaintiff experts defending the reasonableness of treatment are making the same argument in the opposite direction.
Standard of care evidence also determines what future treatment is projectable as damages. A future care projection that includes procedures a competent pain management specialist would not have recommended — or would have performed differently — is vulnerable to a standard of care challenge that will reduce the projected damages. A future care plan grounded in the standard of care for the patient's documented condition is far more defensible. Where the claim also includes non-economic damages, the objective clinical documentation required to meet the standard of care intersects with the evidentiary connection requirement governing pain and suffering awards — a framework examined in the context of Texas personal injury law in the Gregory v. Chohan pain and suffering damages guide.
Understanding the standard of care framework is therefore not optional for attorneys handling pain management litigation. It determines what claims survive summary judgment, what experts are qualified to testify, what treatment is compensable as damages, and what future care projections are recoverable at trial.
Standard of Care vs. Medical Necessity
Standard of care and medical necessity are related but analytically distinct questions. Attorneys who conflate them invite avoidable problems at deposition and trial. For a detailed analysis of how these two concepts operate independently in the same case, see the article on what is the difference between medical necessity and standard of care.
Medical necessity is a threshold determination: was this treatment clinically indicated for this patient's documented diagnosis? It asks whether the intervention was warranted at all — whether the diagnosis supported the proposed treatment, whether conservative measures were trialed first, and whether the selected modality was within the published indications for the condition.
Standard of care is a performance determination: given that the treatment was undertaken, was it performed in conformity with accepted clinical practice? It asks whether the physician who ordered, planned, and executed the treatment did so in the manner a competent specialist would have, addressing technique, dosing, image guidance, patient selection, documentation, informed consent, and complication management.
A procedure can be medically necessary but performed below the standard of care — the injection was indicated, but the physician failed to use fluoroscopic guidance and caused a complication. A procedure can also be performed flawlessly but not indicated — the technique was impeccable, but the patient's imaging and clinical picture did not support the procedure. An expert opinion must engage each question independently, and opposing counsel will probe the distinction on cross-examination.
Standard of Care vs. Causation
Standard of care and causation are the two essential elements of a medical malpractice claim, and they must be addressed separately even when the same expert addresses both.
Standard of care addresses what the treating physician did or failed to do, measured against accepted clinical practice. It is a backward-looking analysis of the defendant's conduct.
Causation addresses whether the identified deviation from the standard of care — not some other factor — produced the claimed harm. In pain management cases, causation is frequently complex because the patient often had a pre-existing painful condition. The causation analysis must isolate the harm attributable to the departure from the harm attributable to the underlying disease, the natural progression of the condition, or other factors unrelated to the defendant's conduct. For the physician methodology of distinguishing pre-existing degeneration from incident-related worsening — directly relevant where the malpractice harm is alleged to have aggravated a pre-existing spine condition — see the article on pre-existing degeneration vs. aggravation in spine injury cases.
In personal injury cases where causation is also contested at the injury level — whether the accident caused the pain condition — causation analysis at the injury level must be distinguished from causation analysis at the malpractice level. A competent opinion addresses each layer of the causal chain separately. For cases where both injury causation and treatment standard of care are at issue, Dr. Dardashti can structure opinions that address each element without conflating them.
Standard of Care vs. Future Medical Care
Standard of care analysis and future medical care projection are distinct services that frequently arise in the same case. Standard of care addresses what happened in the past — whether historical treatment was appropriate. Future medical care addresses what will happen going forward — what treatment the patient will require and at what cost.
The two analyses intersect in a specific way: the future care plan must reflect the standard of care for the patient's current condition. A future care projection that includes procedures or approaches outside the standard of care for the documented condition — whether because they are not indicated, not evidence-based, or inconsistent with the clinical trajectory — is vulnerable to challenge. Conversely, a future care projection that omits standard-of-care treatment that would be expected for the patient's condition undervalues the claim.
In malpractice cases where negligent treatment has produced an ongoing or permanent condition, the future medical care projection must account for the additional treatment attributable to the negligence — the incremental cost of managing a condition that the deviation produced or worsened — as distinct from the cost of treating the underlying condition the patient would have had regardless.
Standard of Care vs. Independent Medical Evaluation
A standard of care analysis and an independent medical evaluation serve different evidentiary functions, though both may be performed by the same physician expert.
An IME is a structured examination of the claimant or patient, addressing the current clinical status, the diagnosis, causation, maximum medical improvement, and future medical needs. The IME focuses on the patient — their current condition, what produced it, and what care they will require.
A standard of care analysis focuses on the treating physician's conduct — what the physician did, what the applicable standard required, and whether the two were consistent. It is typically a records-based analysis that does not require an in-person examination, because the question is about the defendant physician's decisions, not the plaintiff's current clinical status.
In cases where both are needed — malpractice cases where the plaintiff's current condition is disputed alongside the adequacy of prior treatment — an IME and a standard of care analysis can be combined in a single engagement, with the IME findings informing the harm element of the standard of care analysis.
Establishing the Applicable Standard
Establishing the standard of care applicable to a specific pain management clinical decision is one of the most important steps in the opinion process — and one of the most frequently challenged by opposing counsel. An opinion that asserts a standard without identifying its source is not a reliable expert opinion; it is a bare conclusion.
The applicable standard is established through multiple overlapping sources:
- Specialty society guidelines: Published guidance from the American Society of Interventional Pain Physicians (ASIPP), the American Society of Anesthesiologists (ASA), the American Academy of Pain Medicine (AAPM), and the North American Neuromodulation Society (NANS) establish evidence-based standards for specific procedures. These guidelines are not legally binding, but they represent the consensus of the specialty and are the most commonly cited reference in expert opinions.
- Peer-reviewed literature: Published randomized controlled trials, systematic reviews, and observational studies establish the evidence base for specific procedures and inform the applicable standard. Where multiple studies address the same question, the expert must engage the weight of the evidence, not a single favorable result.
- FDA labeling and device approvals: For neuromodulation devices — SCS, ITP, PNS — FDA-approved indications and labeling establish a baseline that is relevant to the standard of care analysis, particularly in cases involving off-label use.
- Textbooks and reference works: Standard pain management textbooks in use at the relevant time period establish what a reasonably well-informed pain management specialist was expected to know.
- Historical standard: The standard applied must reflect what was accepted at the time the treatment was rendered, not what may be the current or emerging standard. Applying a 2025 standard to a 2019 procedure is a methodological error that undermines the opinion's reliability.
Pain Management Procedures Commonly Reviewed for Standard of Care
The following procedures represent the highest-volume standard of care disputes in pain management litigation. Each has a well-developed body of guidelines, technique standards, and published evidence that governs what constitutes adequate practice.
Epidural Steroid Injections
Epidural steroid injections (ESIs) are among the most commonly performed pain management procedures and generate a significant proportion of pain management malpractice claims. Standard of care issues arising in ESI cases include:
- Image guidance: Whether fluoroscopic or CT guidance was used, and whether the applicable standard for the procedure type and approach (interlaminar, transforaminal, caudal) required it.
- Contrast injection: Whether contrast was injected before the steroid to confirm needle position and exclude intravascular placement — a critical standard in transforaminal procedures where the risk of particulate embolism is highest.
- Particulate vs. non-particulate steroid: Whether the steroid formulation selected was appropriate for a transforaminal approach, where particulate steroids carry a documented risk of spinal cord infarction.
- Patient selection: Whether the patient's imaging findings, clinical presentation, and comorbidities were appropriate for the planned procedure, and whether contraindications were evaluated and documented.
- Frequency: Whether the number of injections in a given period exceeded guideline-based limits without documented clinical rationale.
- Complication management: Whether post-procedural complications — including neurological deficits, infection, hematoma, or medication reaction — were recognized and managed appropriately.
Medial Branch Blocks and Radiofrequency Ablation
Medial branch blocks (MBBs) and radiofrequency ablation (RFA) are performed in sequence — the diagnostic MBB series is required before proceeding to RFA, and the standard of care is specific about how each step must be documented. Standard of care issues include:
- Diagnostic block sequencing: Whether the required number of diagnostic medial branch blocks was performed before RFA, and whether the percentage of pain relief from each block was documented and met the published threshold.
- Targeting accuracy: Whether the medial branch target was confirmed with imaging, whether the correct levels and laterality were treated, and whether the lesion was placed at the appropriate anatomic landmark.
- Sensory and motor testing: Whether sensory and motor testing was performed before RFA to confirm appropriate probe placement and exclude motor nerve involvement.
- Repeat ablation interval: Whether repeat RFA was performed at an appropriate interval, with documented rationale, and with re-establishment of the diagnostic response after the prior ablation effect had waned.
- Complication recognition: Whether post-procedure neurological symptoms, dysesthesia, or unexpected pain were appropriately investigated and managed.
Spinal Cord Stimulation
Spinal cord stimulation (SCS) cases represent some of the highest-stakes pain management standard of care disputes because of the procedure's complexity, the cost of complications, and the severity of potential harm including spinal cord injury and infection. Standard of care issues include:
- Patient selection: Whether the indication was supported — typically post-laminectomy syndrome, CRPS, refractory radiculopathy — and whether the failure-of-conservative-care requirement was documented before escalating to neuromodulation.
- Psychological screening: Whether a pre-implant psychological evaluation was obtained and whether identified psychological contraindications were addressed before proceeding.
- Trial adequacy: Whether the trial stimulation period was of adequate duration, whether trial leads were placed appropriately to evaluate the target territory, and whether the trial response was documented with validated outcome measures.
- Implant technique: Whether the permanent implant procedure was performed with appropriate image guidance, lead placement technique, and anchoring — and whether the surgical field was prepared and closed in a manner consistent with infection prevention standards.
- Infection management: Whether post-implant infection — one of the most serious complications of SCS — was recognized promptly, whether appropriate cultures and imaging were obtained, and whether explantation was performed when indicated.
- Lead migration management: Whether lead migration was recognized on follow-up, whether appropriate re-programming was attempted, and whether revision surgery was indicated and appropriately offered.
- MRI compatibility documentation: Whether patients were counseled on MRI restrictions applicable to their specific device, and whether subsequent MRI scans were performed with appropriate precautions.
Intrathecal Pump Therapy
Intrathecal pump therapy (ITP) involves ongoing management of an implanted drug delivery system, and standard of care claims arise not only from implantation but from the long-term management of the device and the medication it delivers. Standard of care issues include:
- Patient selection: Whether the Polyanalgesic Consensus Conference (PACC) patient selection criteria were met, including documentation of systemic opioid trial failure, an adequate trial-to-permanent transition, and absence of absolute contraindications.
- Intrathecal trial: Whether an intrathecal drug trial was conducted, whether the trial methodology was appropriate, and whether the trial demonstrated the required response before proceeding to permanent implantation.
- Drug dosing and titration: Whether the intrathecal drug concentration and dose were within published safety guidelines, whether titration followed PACC-recommended increments, and whether dose escalation was clinically justified and documented.
- Catheter tip granuloma: Whether there was awareness of the risk of catheter tip granuloma — an inflammatory mass at the catheter tip that can cause spinal cord compression — whether appropriate monitoring was in place, and whether new neurological symptoms prompted timely investigation with imaging.
- Drug refill practice: Whether refill procedures followed aseptic technique, whether the correct drug and concentration were confirmed before each refill, and whether the pump was interrogated before refill to confirm residual volume.
- Device end-of-life management: Whether patients were counseled on battery life, whether elective replacement indicators were recognized, and whether device replacement was performed before battery depletion caused abrupt drug withdrawal.
Peripheral Nerve Stimulation
Peripheral nerve stimulation (PNS) raises standard of care questions in a more evolving evidentiary landscape. The applicable standard addresses:
- Indication: Whether the documented neuropathic pain condition was an established indication for PNS at the time of the procedure, distinguishing between indications supported by published evidence and applications that were not yet accepted at the standard of care level.
- Target identification: Whether the peripheral nerve target was identified with appropriate clinical and imaging precision, and whether the electrode placement was confirmed to be in the correct anatomic location.
- Trial period: Whether an adequate percutaneous trial was conducted before permanent implantation, with documented paresthesia coverage of the pain territory and quantified pain relief.
- Infection and lead management: Whether the implant site was managed in a manner consistent with implantable device infection prevention standards, and whether lead-related complications were recognized and addressed.
Documentation Requirements for Standard of Care Analysis
A standard of care analysis is only as reliable as the documentation on which it is based. Inadequate documentation is itself a standard of care finding in many pain management cases. The following records are required for a complete analysis:
- Office visit notes: The complete set of treating physician notes covering the period in question, including history, physical examination findings, assessment, plan, and prescription records.
- Procedure records: Operative reports, fluoroscopy logs and images, anesthesia records, implant operative notes, and post-procedure monitoring records for each procedure at issue.
- Informed consent documentation: Signed consent forms, procedure-specific consent, and any records reflecting that risks and alternatives were discussed with the patient before the procedure.
- Diagnostic imaging: All imaging studies with their reports — MRI, CT, X-ray, bone scan, EMG/nerve conduction studies — relevant to the clinical decisions at issue.
- Complication and incident records: Emergency department records, urgent care visits, hospital admissions, or incident reports related to the adverse outcome being evaluated.
- Device records: For SCS, ITP, and PNS cases — manufacturer field representative records, device programming records, pump interrogation logs, and device end-of-life notifications.
- Pharmacy records: Full prescription history relevant to opioid prescribing cases, including prescription drug monitoring program (PDMP) query records.
- Prior peer review or quality assurance records: Where available, internal hospital or group practice peer review records, credentialing decisions, or quality committee records relating to the treating physician's practice.
- Deposition transcripts: Depositions of the treating physician, facility personnel, and other treating providers that explain the clinical reasoning behind the decisions at issue.
Evidence-Based Medicine and Clinical Guidelines
Pain management practice is more thoroughly governed by published, evidence-based guidelines than most medical specialties. The density of published guidance on specific procedures — particularly interventional procedures — means that standard of care deviations are often documentable with reference to specific guideline provisions, not merely general medical standards.
The principal guideline sources applicable to pain management standard of care analysis include:
- ASIPP Evidence-Based Guidelines: The American Society of Interventional Pain Physicians publishes procedure-specific evidence reviews covering epidural injections, facet joint interventions, radiofrequency procedures, intrathecal therapies, and neuromodulation. These are among the most cited guidelines in pain management litigation.
- PACC Consensus Statements: The Polyanalgesic Consensus Conference provides authoritative guidance on intrathecal drug delivery patient selection, drug selection, dosing, and complication management. PACC statements are the standard reference in ITP cases.
- NANS Practice Guidelines: The North American Neuromodulation Society publishes patient selection and implant practice guidelines for SCS and PNS that establish what a competent neuromodulation specialist is expected to do.
- ASA Practice Guidelines: The American Society of Anesthesiologists publishes guidelines on chronic pain management, acute pain management, and regional anesthesia that provide standards applicable to procedures at the intersection of anesthesiology and pain management.
- CDC Opioid Prescribing Guidance: For opioid prescribing cases, the CDC's clinical practice guideline for prescribing opioids for outpatient chronic pain defines a standard that courts and practitioners in most jurisdictions have accepted as representative of the applicable standard of care.
- California Medical Board Guidelines: The Medical Board of California has published guidance on chronic pain management and opioid prescribing that constitutes a California-specific standard relevant to cases involving California-licensed physicians.
An expert opinion that does not engage the applicable guidelines — that asserts a standard without citing its evidentiary basis — is not a reliable opinion. Opposing counsel will use the absence of guideline grounding as a basis for both Daubert and foundational challenges at trial.
Deviation From Standard of Care
Identifying a deviation from the standard of care is not the same as identifying a bad outcome. Pain management procedures carry known risks, and adverse outcomes occur even when a competent physician performs a procedure correctly. A standard of care deviation is a specific departure from an identifiable clinical standard — not merely an outcome that was unfavorable to the patient.
Deviations in pain management cases typically fall into one of several categories:
- Technical deviations: Failures in procedural technique — incorrect needle placement, failure to use required image guidance, use of contraindicated materials, inadequate confirmation of lead position before ablation.
- Indication failures: Performing a procedure without an established clinical indication — RFA without adequate diagnostic block documentation, SCS implantation without psychological screening, ITP without a documented intrathecal trial.
- Documentation failures: Failure to document informed consent, failure to record the percentage of pain relief from diagnostic blocks, failure to document the clinical rationale for proceeding to a more invasive intervention.
- Complication recognition failures: Failure to recognize the signs and symptoms of a developing complication — infection, hematoma, granuloma, neurological deficit — and failure to investigate or treat the complication appropriately.
- Prescribing failures: Failure to consult PDMP records before prescribing controlled substances, prescribing in the face of documented diversion or aberrant behaviors, failure to conduct required urine drug screening, prescribing doses that exceed guideline-based thresholds without documented clinical rationale.
- Failure to refer: Failure to recognize when a patient's condition, complication, or clinical trajectory exceeded the treating physician's expertise and required referral to a more specialized provider.
Common Allegations in Medical Malpractice Cases
The most frequently encountered standard of care allegations in pain management malpractice litigation involve the following categories of conduct:
- Wrong-level procedure: Performing an injection, nerve block, or ablation at the incorrect spinal level, either through failure to count levels accurately under fluoroscopy or failure to correlate the imaging anatomy with the clinical indication.
- Intravascular injection: Injecting medication into a blood vessel during an epidural or nerve block procedure, producing a systemic adverse event. The applicable standard requires live fluoroscopic imaging with contrast injection before medication delivery.
- Spinal cord stimulator infection: SCS pocket infection, lead infection, or epidural abscess following implantation — particularly when the infection was not promptly recognized, when the patient was immunocompromised, or when explantation was delayed after infection was identified.
- ITP drug error: Delivering the wrong concentration, wrong drug, or wrong volume during a pump refill procedure — one of the most serious complications in intrathecal drug delivery, capable of causing respiratory depression, coma, or death.
- RFA motor nerve injury: Injury to a motor nerve during radiofrequency ablation due to inadequate sensory and motor testing before lesioning, or due to electrode placement outside the intended medial branch target.
- Opioid-related harm: Overdose, death, or addiction-related harm in the context of chronic opioid prescribing that deviated from the applicable prescribing standard — including failure to use PDMP, failure to monitor, or prescribing in the face of documented warning signs.
- Failure to diagnose SCS complication: Failure to identify lead migration, epidural hematoma, or granuloma formation in a timely manner, resulting in delayed treatment and avoidable neurological injury.
Common Allegations in Personal Injury Litigation
In personal injury cases — where the plaintiff's treating physicians are not defendants but their clinical decisions are contested — the standard of care framework is applied to evaluate whether the treatment rendered was appropriate, excessive, or inadequately performed. Common issues include:
- Overtreatment: Defense experts argue that the treating physician performed more procedures than the clinical condition warranted — serial injection series beyond guideline-based frequency limits, premature escalation to device-based care, or continuation of interventional treatment despite documented lack of response.
- Premature surgical escalation: The argument that a conservative treatment course was bypassed in favor of expensive interventional or surgical care before the clinical trajectory supported it.
- Documentation of treatment rationale: The argument that the treating physician's records do not reflect the clinical reasoning that would support the procedures performed — that the records show procedures were ordered without documentation of the indication, the prior treatment failure, or the specific clinical finding that justified the intervention.
- Guideline non-compliance: The argument that the treating physician performed procedures in a manner inconsistent with published guidelines — ESI series exceeding recommended frequency, RFA without adequate diagnostic block documentation, SCS implantation without required psychological screening.
- Appropriate future care standard: The argument that the future care projection reflects a treatment plan exceeding the standard of care for the documented condition, projecting procedures that would not be recommended by a competent pain management specialist.
Device Selection and Neuromodulation Cases
Neuromodulation cases — involving spinal cord stimulation, intrathecal pump therapy, or peripheral nerve stimulation — generate some of the most complex and highest-stakes standard of care disputes in pain management. Several device-specific issues arise that do not appear in injection-based or medication-based cases:
- Device selection: The standard of care requires matching the device to the indication, the patient's anatomy, and the clinical goals. A physician who selects an SCS system incompatible with the patient's imaging needs — for example, a non-MRI-conditional system for a patient likely to require future imaging — may deviate from the applicable standard.
- Programming adequacy: After implantation, adequate programming is required to achieve therapeutic stimulation coverage and optimize device settings. Failure to adjust programming in response to inadequate paresthesia coverage, patient complaints, or program drift is a recognized standard of care issue.
- Revision decision-making: The standard of care requires a structured decision process for revision surgery — confirming that hardware failure, lead migration, or inadequate coverage is the cause of device failure before recommending surgical revision.
- Battery and device end-of-life: Physicians managing implanted devices are expected to monitor battery status, communicate elective replacement indicators to patients, and plan replacement before battery depletion causes unplanned drug withdrawal (ITP) or loss of therapeutic stimulation (SCS).
- Off-label use: When a device is used in an off-label application — for an indication not included in the FDA labeling — the standard of care requires that the off-label use be supported by an established evidence base, that the patient was informed of the off-label status, and that the indication was otherwise clinically appropriate.
Catastrophic Injury Cases
Standard of care analysis in catastrophic injury cases — including spinal cord injury, severe Complex Regional Pain Syndrome, major limb loss with phantom limb pain, or severe neuropathic injury following surgical complication — requires engagement with clinical decisions across multiple specialties and over extended treatment periods. For the standard of care and causation framework specific to CRPS litigation, see the CRPS expert witness guide.
The specific standard of care issues in catastrophic pain management cases include:
- Interdisciplinary coordination: Whether the treating pain management specialist coordinated appropriately with neurosurgery, physiatry, psychiatry, and other relevant specialties in managing a complex, multi-system condition.
- Recognition of emerging complications: Whether a catastrophic complication — such as spinal cord compression from an epidural hematoma or ITP granuloma, or irreversible neurological deficit from a malpositioned SCS lead — was identified at the earliest clinically possible time.
- Documentation across providers: Whether the treating physician's documentation adequately captured a complex clinical picture involving multiple providers, ensuring continuity of care and avoiding communication failures that contributed to the adverse outcome.
- Long-term opioid management in catastrophic cases: Whether the treating physician's opioid management over an extended period met the applicable standard, including monitoring, dose adjustments, and management of opioid-related adverse effects in patients with limited mobility and altered physiology.
Defense Perspective
Defense attorneys retaining a pain management standard of care expert are typically seeking one or more of the following opinions:
- That the defendant physician's conduct was within the standard of care for the specific procedures performed and clinical decisions made — that what was done was consistent with what a competent specialist would have done.
- That the adverse outcome — even if acknowledged — was a known and accepted risk of a procedure performed within the standard of care, and not the result of a departure.
- That the plaintiff's expert has applied an incorrect, unduly strict, or historically inaccurate standard to the defendant's conduct.
- That the causation link between any identified deviation and the claimed harm does not hold — that the harm would have occurred regardless, or that the harm was caused by the underlying condition rather than the treatment.
- In personal injury cases: that the plaintiff's treating physician's care exceeded what the standard of care supports, limiting the compensable treatment to the amount and type that a competent specialist would have recommended.
Dr. Dardashti evaluates these questions honestly from the defense perspective. If the record does not support a standard of care deviation, that opinion is provided. If the record reflects a departure that is not defensible, that assessment is given directly to defense counsel before a written opinion is issued.
Plaintiff Perspective
Plaintiff attorneys retaining a pain management standard of care expert are typically seeking opinions on one or more of the following:
- That a specific, identified act or omission by the defendant physician constituted a departure from the standard of care applicable to a pain management specialist — not a generalized critique, but a specific finding grounded in the published clinical standards.
- That the departure caused a specific harm — neurological injury, drug complication, device failure, delay in appropriate care — distinguishing the harm caused by the deviation from the harm caused by the underlying condition.
- That the defendant's expert has applied an incorrect, overly permissive, or generic standard that does not reflect what the specialty actually requires in the clinical circumstances at issue.
- That the plaintiff's treating physicians' care was within the standard of care for the diagnosed condition — rebutting defense arguments that treatment was excessive, premature, or guideline non-compliant.
- That future care projections reflecting guideline-appropriate treatment for the plaintiff's documented condition are supported by the standard of care and should be fully compensated.
Attorney Retention Scenarios
Standard of care engagements arise in a variety of litigation contexts. The following scenarios represent the most common retention patterns:
- Medical malpractice pre-filing review: Plaintiff counsel retains a pain management standard of care expert before filing to evaluate whether the record supports a viable departure opinion — identifying the specific deviation, the applicable standard, and the causal link before committing to litigation.
- Defense early case assessment: Defense counsel retains a pain management expert early in the case to evaluate whether the defendant's conduct was within the standard of care and to identify the weaknesses in the plaintiff's anticipated expert opinion.
- Rebuttal opinion: Either plaintiff or defense counsel retains an expert to respond to a filed expert opinion — identifying errors in the opposing expert's standard, methodology, or application of the standard to the facts.
- Personal injury treatment defense: Defense counsel retains a pain management expert to evaluate whether the plaintiff's treating physicians' care was within the standard of care, and to testify about what the standard of care supports as compensable treatment.
- Insurance coverage analysis: Insurance carriers or coverage counsel retain a pain management expert to evaluate whether a specific treatment was within the standard of care for coverage purposes — distinct from a medical necessity determination under the policy.
- Deposition and trial testimony: Any of the above engagements may extend to deposition testimony on the standard of care opinion, cross-examination preparation for opposing experts, or trial testimony depending on the case trajectory.
How to Request a Standard of Care Analysis
Contact Expert Medical Services LLC with the case records, the specific procedure or clinical decision at issue, and the standard of care questions to be addressed. For malpractice cases, identifying the alleged deviation at the outset — rather than asking the expert to identify it — allows for a more targeted initial record review. For personal injury cases where treatment appropriateness is in dispute, describing the defense position on the treatment allows the expert to engage the specific critique.
For cases also requiring causation analysis, see the Causation Analysis service. For cases requiring in-person examination, a concurrent Independent Medical Evaluation may be appropriate. For cases where future care projections are also at issue, see the Future Medical Care Review service. For cases requiring physician-level record review and a written opinion without a standard of care question, see the Medical Record Review service.
Standard of care opinions are available as written record review reports, supplemental declarations responding to opposing expert opinions, and deposition or trial testimony. Dr. Dardashti provides opinions for plaintiff and defense counsel, insurance carriers, government agencies, mediators, and courts in California and nationwide.
Related Services & Expertise
Medical Necessity Review
Threshold analysis of whether pain management treatment was clinically indicated for the documented diagnosis.
Future Medical Care Review
Evidence-based projection of future treatment costs once the standard of care framework is established.
Causation Analysis
Linking mechanism of injury to diagnosis — the causal foundation underlying the standard of care dispute.
Independent Medical Evaluation
Structured examination and written opinion addressing diagnosis, causation, standard of care, and future care.
Spinal Cord Stimulation
SCS candidacy, implantation standards, device complications, and standard of care in neuromodulation disputes.
Intrathecal Pump Therapy
ITP patient selection, drug dosing standards, catheter complications, and device management review.
FAQ
Standard of Care Analysis — Common Attorney Questions
- A standard of care analysis is a physician's written opinion on whether the conduct of a treating pain management physician — including diagnostic decisions, procedural choices, technique, documentation, and follow-up — conformed to the standard of practice applicable to a qualified pain management specialist under similar clinical circumstances. In litigation, the standard of care opinion is the evidentiary foundation for establishing whether a deviation occurred and, if so, whether that deviation produced the claimed harm. A pain management standard of care analysis addresses the specific procedures, devices, and clinical decisions at issue in the case — not a generic description of how pain management is practiced.
- Standard of care and medical necessity are analytically distinct questions that frequently arise from the same set of facts. Medical necessity asks whether a procedure was clinically indicated for the patient's documented diagnosis — the threshold question of whether intervention was warranted at all. Standard of care asks whether the physician who performed the procedure did so in a manner consistent with accepted clinical practice — the question of how the treatment was performed. A procedure can be medically necessary but performed below the standard of care. It can also be performed flawlessly while not being indicated in the first place. Both must be addressed independently in any competent expert opinion that touches on treatment appropriateness.
- In California medical malpractice litigation, the applicable standard of care is that degree of care, skill, and treatment which, in light of all relevant surrounding circumstances, is recognized as acceptable and appropriate by reasonably prudent similar health care providers (CACI 501). A pain management specialist is held to the standard of care applicable to pain management specialists — not to general practitioners or to physicians in other specialties. Dr. Dardashti's opinions are structured to articulate the specific standard applicable to the defendant's specialty, the clinical circumstances of the case, and the manner in which the defendant's conduct did or did not conform to that standard.
- Yes. A pain management physician expert can address both the standard of care question — whether the treating physician's conduct deviated from accepted practice — and the causation question — whether that deviation caused the patient's claimed harm. Separating these into two opinions from two experts is sometimes done for tactical reasons, but a single well-organized expert opinion that addresses both elements is often more efficient and more persuasive. Dr. Dardashti structures opinions to address each element independently so that causation findings do not contaminate the standard of care analysis, and vice versa.
- The procedures most frequently at issue in pain management standard of care litigation include epidural steroid injections (intravascular injection, wrong level, inadequate fluoroscopic guidance), medial branch blocks and radiofrequency ablation (incorrect targeting, inadequate diagnostic block sequencing, inappropriate re-ablation interval), spinal cord stimulation (patient selection failures, inadequate trial, lead migration, infection), intrathecal pump therapy (drug dosing errors, catheter complications, failure to recognize granuloma), and opioid prescribing (inadequate monitoring, failure to use prescription drug monitoring programs, prescribing in the face of documented diversion). Each procedure has specific technical and clinical standards that govern what a qualified pain management specialist is expected to do.
- Standard of care is a historical question: what did a reasonably competent pain management specialist know and do at the time the treatment was rendered, not what might be done today under current guidelines. Dr. Dardashti establishes the applicable standard through a combination of specialty society guidelines in effect at the relevant date, peer-reviewed literature published before the event, practice standards documented in published textbooks and continuing medical education materials, and the evolving evidence base as of the treatment date. Applying current guidelines retroactively to historical conduct is a methodological error that opposing experts will challenge; Dr. Dardashti avoids it by anchoring opinions to the appropriate historical standard.
- A complete standard of care analysis requires the full medical record covering the treatment period at issue — office visit notes, procedure records, fluoroscopy images and reports, post-procedure notes, informed consent documentation, medication records, diagnostic imaging with interpreting reports, follow-up notes, and emergency treatment records if complications occurred. For device-based cases — spinal cord stimulation, intrathecal pump therapy — operative reports, device programming records, and device company field representative records are also relevant. Incident reports, facility credentialing records, and prior peer review records may be relevant in cases involving hospital-based procedures. The completeness of the record is itself a standard of care issue in many cases.
- Yes. Opioid prescribing is among the most contested standard of care issues in pain management, and it arises in both malpractice and personal injury contexts. The standard of care analysis addresses whether the prescribing physician complied with California Medical Board guidance on chronic opioid therapy, the CDC clinical practice guideline applicable at the time of prescribing, relevant DEA scheduling and documentation requirements, and the clinical indicators that should have prompted reassessment, referral, or discontinuation. Cases involving prescription drug monitoring program (PDMP) failures, inadequate functional assessment, or prescribing in the face of documented aberrant behaviors are among the most common opioid standard of care disputes.
- An independent medical evaluation (IME) is a structured examination of the claimant or patient — addressing diagnosis, causation, current clinical status, and future medical needs — with or without a standard of care component. A standard of care analysis is typically a records-based review that does not require an in-person examination: the question is about the treating physician's conduct, not the patient's current clinical status. In cases where the standard of care analysis requires an understanding of the patient's current functional status to assess whether harm occurred, an IME and a standard of care analysis may be combined. In most malpractice cases, the standard of care review proceeds from the medical record.
- In federal court under Daubert, and in California state court under Kelly-Frye and its successors, expert opinions must be based on sufficient facts or data, a reliable methodology, and proper application of that methodology to the facts of the case. For pain management standard of care opinions, a reliable methodology includes articulating the specific standard claimed, identifying the published sources that establish that standard, demonstrating that the standard was applicable to the defendant's clinical setting and the patient's condition, and applying that standard to the specific conduct at issue. An opinion that asserts a standard without methodology — or that applies a stricter standard than the published literature supports — is vulnerable to a Daubert challenge that an experienced defense or plaintiff attorney will bring.
- Yes. Pain management procedures performed in academic or training settings raise specific standard of care questions: whether adequate supervision was provided, whether the fellow or resident performing the procedure had reached the competency threshold required for the specific procedure, whether attending oversight was documented, and whether the institution's training program policies were followed. Dr. Dardashti can address the applicable standard for supervised procedures in training settings, the distinction between attending and trainee responsibility, and whether the supervision structure met the standard expected in academic pain management practice.
- Not every adverse outcome in pain management is a departure from the standard of care. Known complications of properly performed procedures — including dural puncture during epidural injection, temporary post-procedural pain flare, or lead migration after spinal cord stimulator implantation — can occur in the absence of any deviation. The standard of care analysis must distinguish between an adverse outcome that occurred despite proper technique and care, and an adverse outcome that resulted from a departure from accepted practice. A plaintiff who suffered a complication does not prevail merely by showing the complication occurred; the standard of care analysis must identify a specific departure — in technique, indication, documentation, informed consent, or follow-up — that caused the outcome.
- Not every clinical decision a physician makes is reducible to a single correct answer. Pain management practice involves clinical judgment — the exercise of professional discretion within a range of acceptable options. A standard of care deviation is a specific departure from what a reasonably competent pain management specialist would have done, not merely a choice of one acceptable option over another. The expert's analysis must distinguish between conduct that falls outside the acceptable range of professional practice and conduct that represents a reasonable clinical judgment that a different competent physician might have made differently. Defense experts frequently invoke 'clinical judgment' to defend conduct that the plaintiff's expert characterizes as a deviation; the key question is whether the conduct in question was within the range of options a reasonably competent specialist would have considered acceptable — not whether it was the ideal choice.
- Yes. Complex Regional Pain Syndrome (CRPS) is one of the most clinically complex and litigation-intensive conditions in pain management, and the standard of care for its diagnosis and treatment is frequently contested. Standard of care issues in CRPS cases include: whether the Budapest Criteria were applied and documented in establishing the diagnosis; whether the sequential treatment ladder — pharmacological, physical, interventional, and neuromodulatory — was followed appropriately; whether spinal cord stimulation was pursued at the appropriate point in the clinical trajectory; and whether the treating physician's documentation supports the clinical decisions made at each treatment stage. CRPS cases often combine standard of care issues with causation and medical necessity disputes that must each be addressed separately.
- The clinical standard of care for pain management procedures is largely national — governed by specialty society guidelines, peer-reviewed literature, and FDA labeling that apply regardless of jurisdiction. However, California introduces jurisdiction-specific layers: the Medical Board of California's guidance on chronic pain management and opioid prescribing establishes a California-specific standard relevant to cases involving California-licensed physicians; the CACI 501 jury instruction defines the applicable standard for California medical malpractice cases; and California's Evidence Code §§ 720 and 801 govern how expert qualifications and opinion foundations are established at trial. For attorneys litigating pain management standard of care cases in California, understanding these jurisdiction-specific dimensions — including how the Sargon admissibility standard applies to expert opinions — is essential to structuring an opinion that will survive pretrial challenge.
Request a Standard of Care Analysis
Available for plaintiff and defense. Contact Expert Medical Services LLC with case records, the treatment at issue, and the specific standard of care questions to be addressed.