Nationwide Pain & Injury Medical Expert Witness
Causation Analysis — Pain Management
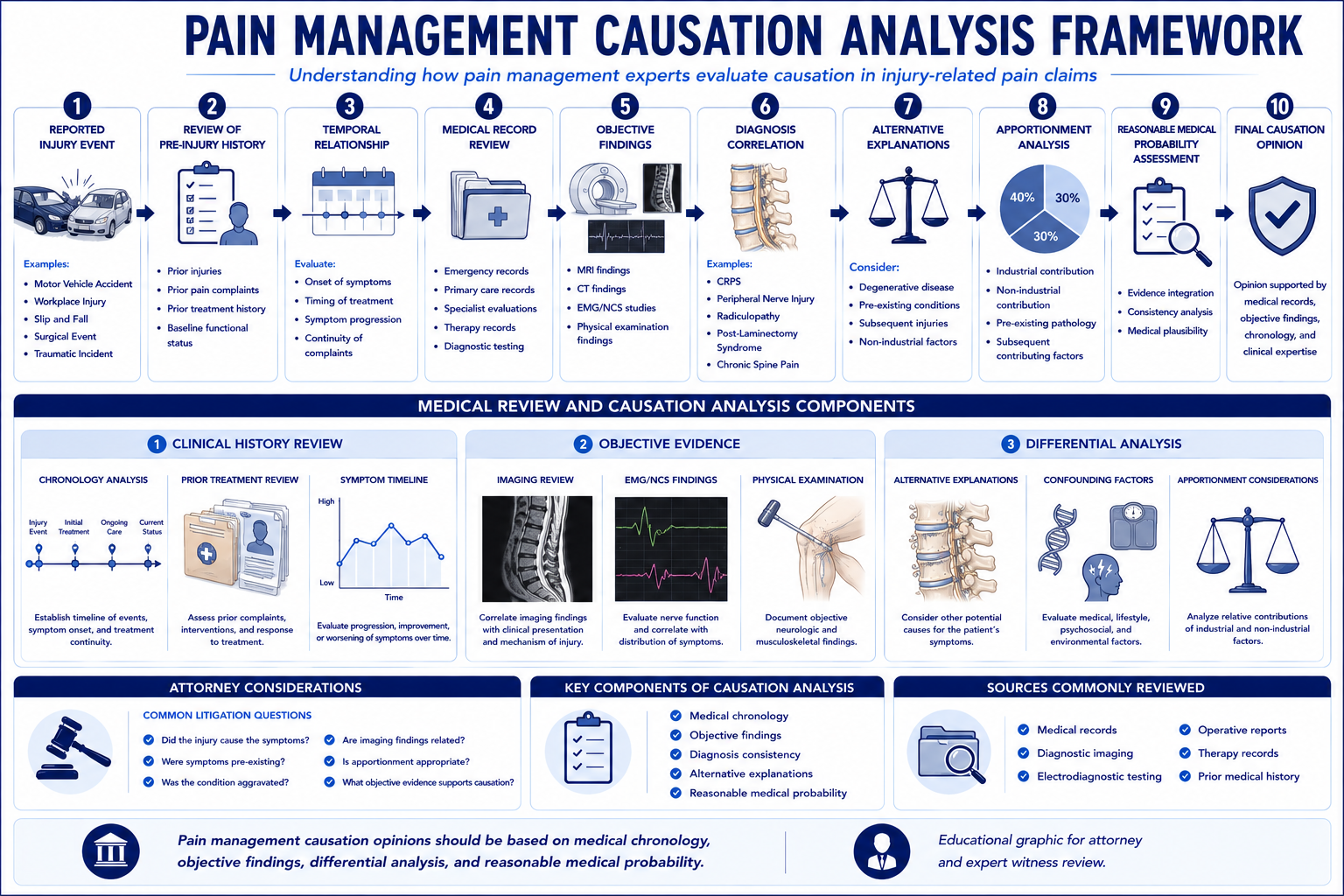
Evidence-based analysis of whether a diagnosed pain condition is causally related to the subject incident. Records review, written opinion, and supplemental declarations for deposition and trial. Plaintiff and defense.
Request AvailabilityCredentials & Qualifications
- Service
- Causation Analysis & Written Opinion
- Specialty
- Pain Management & Anesthesiology
- Standard Addressed
- Substantial Factor & But-For Causation
- Opinion Format
- Written Report, Supplemental Available
- Available For
- Plaintiff & Defense
- Jurisdiction
- State & Federal — Nationwide
What Is Medical Causation?
Medical causation addresses a single foundational question: did the subject event cause — or substantially contribute to — the diagnosed condition? In litigation, establishing causation is not optional; it is the threshold that separates a compensable injury from background disease, natural aging, and prior conditions that would have produced the same symptoms regardless of the incident.
Clinical causation is a physician's judgment about whether a plausible biological mechanism connects the event to the diagnosis. It requires evaluating the mechanism of injury, the temporal onset of symptoms, the pre-incident medical baseline, the findings on physical examination and imaging, and the biological plausibility of the proposed causal pathway. Clinical causation does not require certainty — it requires that the causal connection be supported by the medical evidence to a reasonable degree of medical probability.
Legal causation maps onto the clinical analysis but applies a specific standard: in California personal injury litigation, the applicable standard is substantial factor causation — the subject event must have been a material contributing cause of the condition, even if not the only cause. A pre-existing degenerative condition does not defeat causation if the incident substantially aggravated it. A claimant who had asymptomatic degenerative disc disease before an accident can establish causation for a new symptomatic radiculopathy if the incident produced the aggravation that transformed a subclinical finding into a clinically significant, functionally limiting condition.
Temporal relationship is not causation. The fact that a claimant developed pain after an incident is necessary but not sufficient to establish causation. The expert must address whether the relationship is biologically plausible, whether the mechanism is consistent with the claimed injury, whether the medical record chronology is coherent, and whether alternative explanations have been considered and addressed. Post hoc ergo propter hoc — it happened after, therefore it was caused by — is not a reliable causation opinion and will not withstand cross-examination.
Causation disputes arise in pain management litigation because chronic pain conditions often develop on a substrate of pre-existing degenerative disease, because the conditions most frequently claimed — disc herniation, radiculopathy, facet-mediated pain, CRPS, peripheral nerve injury — do not always produce unambiguous imaging findings, and because the financial stakes of establishing or defeating causation are high in cases involving expensive interventional and device-based treatment. For a detailed discussion of how causation analysis functions in California personal injury matters, see the article on how pain management experts evaluate causation in personal injury cases.
How Pain Management Experts Evaluate Causation
A defensible causation opinion is not a conclusion appended to a record review. It is a structured analytical process that moves from the documented facts to the applicable medical standard to a reasoned conclusion. The following elements constitute the analytical framework a qualified pain management expert applies in every causation engagement.
Mechanism of Injury
The mechanism of injury is the starting point of any causation analysis. The expert evaluates whether the described mechanism — the direction of force, the magnitude of impact, the position of the claimant's body, the nature of the physical event — is biomechanically consistent with the claimed diagnosis. A lumbar compression fracture requires different force vectors than a cervical facet injury; a workplace repetitive-motion injury involves different anatomical stresses than a single-event trauma. The mechanism must be plausible as a cause of the specific diagnosis, not merely as a cause of pain generally.
For motor vehicle accident cases, the available collision data — repair estimates, delta-V calculations, police reports, photographs, and biomechanical analysis — are reviewed in conjunction with the claimant's reported symptoms and the treating record. For workplace injuries, the work tasks, tool use, body position, and ergonomic conditions are evaluated against what is known about the biomechanics of occupational spinal and peripheral nerve injury.
Timing of Symptom Onset
The timing of symptom onset relative to the incident is one of the most important elements of the causation analysis — and one of the most frequently contested. A claimant who reported no symptoms at the scene, sought no treatment for several weeks, and then presented with a complex spinal diagnosis presents a different causation picture than one who went directly to an emergency room with acute neurological symptoms.
The expert evaluates whether the timing is biologically consistent with the claimed causal mechanism. Some injuries produce immediate symptoms; others — including CRPS, certain peripheral nerve injuries, and delayed inflammatory responses — may produce delayed onset that is still consistent with causation. The analysis must address the specific condition's known presentation pattern and explain whether the documented timing supports or undermines the proposed causal relationship.
Medical Records Chronology
The medical record chronology is the evidential backbone of the causation analysis. The expert constructs a detailed timeline: what the claimant's documented medical baseline was before the incident; what the first post-incident medical encounter showed; how symptoms evolved across treating providers; whether the clinical picture is internally consistent; and whether any gaps, inconsistencies, or changes in the claimed symptom pattern require explanation.
The pre-incident record is as diagnostically important as the post-incident record. Prior complaints involving the same anatomical region, prior imaging showing the same structural findings, prior treatment for overlapping conditions — all must be evaluated to determine whether the post-incident presentation represents a new condition, an aggravation of a pre-existing one, or a continuation of an ongoing clinical process. Records from five to ten years before the incident may be relevant in degenerative spine cases.
Physical Examination Findings
Physical examination findings provide the objective clinical anchor for the causation determination. For spinal conditions, the expert evaluates whether documented examination findings — dermatomal sensory loss, motor deficits, positive provocative tests, reflex changes, range-of-motion limitations — are consistent with the claimed diagnosis and the proposed causal mechanism. Examination findings that are inconsistent with the claimed anatomical level, that fluctuate implausibly, or that are absent when the diagnosis requires them are relevant to the causation analysis. For the full examination methodology — including validated functional instruments, imaging correlation, and symptom validity assessment — see the article on how pain management experts objectively evaluate pain.
For neuropathic conditions including CRPS and peripheral nerve injury, examination findings may be the primary objective evidence available. The presence or absence of vasomotor changes, trophic changes, allodynia, hyperalgesia, and temperature asymmetry are diagnostically critical and directly relevant to both causation and the Budapest Criteria analysis for CRPS.
Imaging Correlation
Imaging findings must be interpreted in the context of causation, not treated as self-explanatory evidence. The expert evaluates whether the imaging findings are consistent with the mechanism of injury, whether they correspond to the symptomatic level and side, whether they represent new post-incident pathology or pre-existing degenerative changes, and whether the imaging evolution over time is consistent with the claimed clinical trajectory.
Degenerative findings on post-incident imaging — disc space narrowing, osteophytes, facet joint hypertrophy, loss of disc signal — are common in the general population and frequently predate the incident at issue. The expert must distinguish between degenerative findings that reflect decades of natural aging and post-traumatic changes — acute disc herniation, new endplate injury, acute ligamentous disruption, bone marrow edema — that are more directly attributable to the incident. When pre-incident imaging is available, direct comparison is essential.
Functional Changes
Causation is not limited to the diagnosis itself — it extends to the functional consequences of the diagnosis. The causation analysis evaluates whether the documented functional changes — limitations in activities of daily living, work capacity, ambulation, and functional performance — are consistent with the claimed diagnosis, are attributable to the incident, and represent a change from the claimant's pre-incident functional baseline.
Documented functional changes that significantly predate the incident — disability filings, Social Security disability applications, or records showing functional limitations from conditions unrelated to the incident — must be accounted for in the causation analysis. The expert must distinguish the functional deficit attributable to the incident from the functional baseline the claimant would have experienced absent the event. For how objective functional evidence connects to non-economic damages under the rational evidentiary connection requirement in Texas personal injury law, see the Gregory v. Chohan pain and suffering damages guide.
Alternative Explanations and Differential Causation
A causation opinion that does not address alternative explanations is an incomplete opinion. The expert must identify the plausible competing explanations for the claimant's condition — including natural disease progression, prior unrelated injuries, occupational exposure, lifestyle factors, and other medical conditions — and explain why the proposed causal mechanism is more likely than the alternatives given the specific facts of the case. This differential causation analysis is the equivalent of a clinical differential diagnosis applied to the legal causation question: ruling in the proposed cause and ruling out the alternatives with reference to the documented evidence.
Aggravation of Pre-Existing Conditions
The aggravation doctrine is one of the most practically important concepts in pain management causation analysis. The defendant takes the plaintiff as they find them: a claimant with pre-existing degenerative disc disease, prior spinal surgery, or prior injury is still entitled to compensation if the subject incident materially aggravated a pre-existing condition into a more severe, more symptomatic, or more functionally limiting state.
Degenerative Spine Disease
Degenerative changes of the cervical and lumbar spine are ubiquitous in the adult population and are present on imaging in a majority of adults over forty regardless of any injury history. The presence of degenerative findings on post-incident imaging does not defeat causation — it requires the expert to distinguish between findings that reflect cumulative degeneration and findings that represent acute traumatic changes superimposed on a degenerative background. An acute disc herniation at a level with pre-existing degenerative disc disease is causally attributable to the incident if the mechanism of injury is consistent with disc herniation and the pre-incident record does not document prior symptomatic herniation at that level.
Prior Injuries at the Same Site
Prior injuries to the same anatomical region require a more nuanced analysis. The expert must evaluate what clinical status the claimant had reached following the prior injury — whether they had reached maximum medical improvement, what residual symptoms remained, what the treatment trajectory was immediately before the current incident — and determine what new or worsened condition the current incident produced beyond that baseline. The relevant question is not whether the prior injury was present, but whether the current incident produced a material change in clinical status relative to the pre-incident condition.
Asymptomatic vs. Symptomatic Pre-Existing Conditions
The distinction between asymptomatic and symptomatic pre-existing conditions is significant in the causation analysis. A pre-existing condition that was producing documented symptoms before the incident provides a less clean baseline for the causation argument — the expert must explain what change the incident produced beyond the pre-existing symptom pattern. An asymptomatic pre-existing condition that is activated by the incident into a symptomatic state supports a causation finding even without any prior treatment record for that condition, as long as the imaging documentation of the pre-existing pathology and the absence of prior symptom documentation is established. For a physician's methodology on applying this distinction in spine injury cases, see the article on pre-existing degeneration vs. aggravation in spine injury cases.
Acceleration vs. Aggravation
Acceleration refers to a condition that would have deteriorated to its current state through the natural history of the underlying disease, but has reached that state earlier than it would have absent the incident. Aggravation refers to a worsening of the condition beyond what the natural history would have produced — a more severe or more symptomatic state than would have occurred without the trauma. Both are compensable, but they produce different damages analyses: an acceleration claim focuses on the value of the time period by which disease progression was hastened; an aggravation claim focuses on the incremental severity and functional impairment produced by the incident beyond the natural history trajectory.
Objective Findings and Causation by Condition
The causation framework applies differently depending on the specific pain condition at issue. Each diagnosis has characteristic objective findings, imaging correlates, and a known natural history that shapes the causation analysis.
Disc Herniation and Radiculopathy
Post-traumatic disc herniation is one of the most frequently litigated causation issues in pain management. The key elements of the analysis are: whether the mechanism of injury is consistent with disc herniation (axial loading, sudden flexion-extension, rotational force); whether post-incident imaging shows new herniation or a herniation change from pre-incident imaging; whether the clinical presentation includes dermatomal radicular symptoms consistent with the level of herniation; and whether the examination findings include neurological deficits that correspond to the imaged level. Defense experts frequently argue that the herniation represents naturally occurring degenerative protrusion rather than traumatic disc disruption — the causation analysis must engage this argument with reference to the imaging characteristics that distinguish traumatic from degenerative disc herniation.
Complex Regional Pain Syndrome
CRPS causation requires a two-step analysis: first establishing that the Budapest Criteria are satisfied (confirming the diagnosis), then establishing that the triggering event produced the condition. CRPS can be triggered by trauma, surgical procedures, fractures, soft tissue injury, and peripheral nerve injury — all of which may arise from the incidents typically at issue in personal injury litigation. The causation expert addresses whether the claimant's documented examination findings satisfy the Budapest Criteria, whether the onset pattern is temporally consistent with CRPS development following the triggering event, and whether alternative diagnoses have been appropriately considered. For a detailed discussion of CRPS in litigation, see the CRPS expert witness guide.
Peripheral Nerve Injury
Peripheral nerve injury from traction, compression, or direct trauma requires the causation analysis to establish: the mechanism by which the incident could produce the specific nerve injury claimed; the nerve distribution of the reported symptoms; the electrodiagnostic findings (EMG/nerve conduction studies) that confirm nerve injury; and the temporal relationship between the incident and the onset of neuropathic symptoms. The expert must distinguish traumatic peripheral nerve injury from entrapment neuropathies, diabetic peripheral neuropathy, and other conditions that produce similar symptoms but are unrelated to the incident.
Post-Laminectomy Syndrome
Post-laminectomy syndrome — persistent pain following spinal decompression or fusion surgery — raises a distinct causation question: whether the surgery itself, the decision to operate, and the clinical trajectory that led to surgery were causally attributable to the subject incident. The causation analysis must trace the chain from the incident to the diagnosis that indicated surgery, to the surgical procedure, to the post-surgical pain state. If the surgery was medically necessary as a direct consequence of the incident-related injury, the post-surgical pain condition is causally linked to the incident through that chain.
Cauda Equina Syndrome
Cauda equina syndrome — compression of the cauda equina nerve roots producing bladder, bowel, and lower extremity dysfunction — is one of the most severe spinal pain conditions in litigation, arising from traumatic disc herniation, epidural hematoma following spine surgery, or procedural complications. The causation analysis addresses the mechanism of compression, the timing of presentation, whether the treating record reflects timely recognition and intervention, and whether delayed treatment contributed to permanent neurological deficit — raising both causation and standard of care questions in the same case.
Common Causation Disputes
The following causation scenarios represent the most frequently contested issues in pain management litigation. Understanding each dispute pattern allows attorneys to evaluate their causation evidence and identify the expert analysis needed before retaining.
- Delayed treatment: The claimant did not seek medical care immediately following the incident and presented for treatment days, weeks, or months later. The defense argues that the delay reflects an absence of significant injury. The causation expert addresses whether the delay is consistent with the biology of the claimed condition, whether social, financial, or access-to-care factors explain the delay, and whether the condition documented at the first medical encounter is consistent with an injury of the claimed vintage.
- Gaps in care: Periods of non-treatment after initial care are used by the defense to argue that the condition resolved or was not as severe as claimed. The causation expert evaluates whether the gap is consistent with episodic or intermittent symptoms, whether the clinical presentation at return-to-care is consistent with the prior diagnosis, and whether the gap reflects clinical improvement, financial barriers, insurance lapses, or patient decision-making rather than condition resolution.
- Minor impact collisions: Low-speed vehicle impacts where damage is minimal are among the most contested causation scenarios. Defense biomechanical experts argue that the impact forces were below the threshold for tissue injury. Causation experts counter with the published biomechanical literature on occupant kinematics, the role of pre-existing spinal vulnerability in force amplification, and the absence of a reliable linear relationship between vehicle damage and occupant injury. The analysis must engage the specific collision parameters rather than relying on generic impact-velocity arguments.
- Subsequent accidents: When the claimant is involved in a subsequent accident after the incident at issue, the defense argues that the subsequent event, rather than the original incident, caused or substantially contributed to the current condition. The causation expert addresses the clinical status between the incidents — what was documented before the second event — and what new injury or worsening the second incident produced. Apportionment between incidents requires careful chronological analysis of the treating record.
- Multiple injury events: Claimants with multiple prior injuries or accident histories require the expert to address each contributing event and its individual causal contribution to the current condition. The analysis must produce a coherent account of the cumulative picture while maintaining analytical precision about what each event contributed. This is among the most complex causation analyses and requires comprehensive record assembly covering the full prior injury history.
- Pre-existing degeneration without prior symptoms: Imaging showing multi-level degenerative disc disease in the absence of a prior treatment record is a common defense argument against causation. The expert addresses whether the imaging appearance is consistent with long-standing degenerative disease or with a more recent process, whether the clinical onset pattern is consistent with acute trauma superimposed on degenerative disease, and whether the absence of prior treatment reflects the absence of prior symptoms or a gap in the medical record.
Plaintiff and Defense Perspectives
Plaintiff Arguments
Plaintiff causation experts establish the biological plausibility and evidentiary support for the causal link between the incident and the diagnosis. The core arguments are: that the mechanism of injury is consistent with the documented diagnosis; that the temporal relationship between the event and the onset of symptoms is medically coherent; that the pre-incident record documents the absence of the claimed condition or a materially different clinical baseline; that the imaging and examination findings are consistent with the proposed causal mechanism; and that the alternative explanations advanced by the defense have been considered and do not adequately account for the documented clinical picture.
For aggravation cases, the plaintiff expert establishes that the incident produced a material change in clinical status — a new symptom pattern, a functional decline, a worsened imaging finding, or an escalation in treatment — that distinguishes the post-incident condition from the pre-incident baseline. The argument is not that the pre-existing condition was irrelevant, but that the incident caused a specific and identifiable change beyond the natural history of the underlying disease.
In California personal injury cases, the plaintiff causation expert structures the opinion within the substantial factor framework — establishing that the incident was a material contributing cause of the current condition, not the sole cause, and that the pre-existing disease does not defeat causation under the applicable legal standard. For California-specific discussion of how causation expert opinions interact with Evidence Code admissibility requirements and jury instruction frameworks, see the California pain management expert witness guide.
Defense Arguments
Defense causation experts attack the weakest links in the causal chain — the elements of the plaintiff's causation theory that the medical record does not fully support. The most effective defense arguments are specific and record-anchored: a temporal gap that is inconsistent with the claimed diagnosis; an imaging finding that predates the incident based on documented prior imaging; an examination finding that is inconsistent with the alleged anatomical lesion; or a prior treatment record that shows the claimant was already receiving care for the claimed condition before the accident.
Defense experts also raise structural arguments about the causation framework: that the mechanism of injury is not biomechanically consistent with the severity of the claimed injury; that the natural history of the claimed condition does not support the duration and severity of the treatment that followed; and that the treating physician's documentation fails to address the causation question with the specificity needed to establish it as a compensable claim rather than a coincident condition.
Rebuttal Analysis
When a defense causation opinion has been produced, a targeted rebuttal identifies the specific clinical arguments that are inconsistent with the complete record, the biomechanical literature, or the applicable medical standards. Effective rebuttal does not repeat the original causation opinion — it engages the defense expert's specific arguments, identifies what the defense expert did not address or mischaracterized, and explains where the defense expert's analysis departs from the weight of the relevant evidence.
Rebuttal opinions are particularly important in cases where the defense expert reviewed a limited set of records, applied a biomechanical analysis without adequate clinical grounding, or assessed causation without examining the complete pre-incident medical history. A rebuttal that engages these gaps specifically — rather than simply reasserting the original causation conclusion — is far more effective at deposition and trial than one that recycles the original opinion in different language.
Causation and Medical Necessity
Causation and medical necessity are related but analytically distinct questions that must each be addressed with physician-level specificity. Causation asks: did the incident produce the condition? Medical necessity asks: given the condition — however it arose — was the treatment rendered or proposed clinically warranted?
Both issues arise in most personal injury cases, and both must be answered to resolve the damages question. A defense expert who concedes causation but challenges medical necessity forces the plaintiff to defend each treatment decision on its clinical merits. A plaintiff expert who establishes causation but cannot defend the necessity of expensive interventional or device-based care is vulnerable on the damages side. The two analyses must be coherent — the necessity determination must be grounded in the same diagnosis that the causation analysis establishes, and the causal chain must extend from the incident to the specific treatment claimed as damages.
Causation and Future Medical Care
Causation establishes the perimeter of compensable future medical care. Treatment that is causally attributable to the subject incident is recoverable as future damages; treatment for conditions unrelated to the incident or for the natural progression of pre-existing disease that would have been required regardless is not. In practice, the causation analysis must be substantially complete before future care projections can be properly scoped — the projected treatment must be grounded in the diagnosed condition, and that condition must be attributable to the incident.
For cases involving high-cost future care — spinal cord stimulation, intrathecal pump therapy, or long-term neuromodulation management — the causation analysis for each projected treatment item must be explicitly addressed. A future care projection that includes SCS without establishing that the underlying condition necessitating neuromodulation is causally attributable to the incident will not withstand expert challenge. The future medical care review and causation analysis can be performed as a coordinated engagement, with each opinion structured to reinforce the other.
When causation is also contested at the standard of care level — where the treatment itself is alleged to have produced an additional injury — the causal chain becomes multi-layered. A pain management physician can address both the injury causation question and the treatment causation question in a structured opinion that keeps each layer analytically distinct. For these cases, see the standard of care analysis service page.
Documentation Required for Causation Analysis
A complete causation analysis requires the following record categories:
- Pre-incident medical records: Treatment records, imaging studies, pharmacy records, and prior claim history from before the subject incident — ideally five to ten years, or further if prior injuries to the same region are claimed. The pre-incident record establishes the medical baseline against which the causation analysis is measured.
- Incident documentation: Police reports, accident reconstruction reports, workplace incident reports, and available photographic or video evidence of the incident mechanism.
- Emergency and acute care records: Emergency department records, urgent care visits, and any imaging obtained in the immediate aftermath of the incident.
- Treating physician notes: All notes from pain management physicians, orthopedic surgeons, neurosurgeons, neurologists, physiatrists, and primary care physicians from the post-incident period.
- Diagnostic imaging: MRI, CT, X-ray, bone scan, and EMG/nerve conduction studies, with the interpreting reports. Pre-incident imaging for comparison when available.
- Procedure and operative records: All interventional procedure records, surgical operative reports, and device implantation records.
- Deposition transcripts: Depositions of the claimant, treating physicians, and any prior expert witnesses that address the causation question.
- Opposing expert reports: For rebuttal engagements, the opposing causation expert's written report and any supplemental declarations.
How to Request a Causation Analysis
Contact Expert Medical Services LLC with the case summary, the incident mechanism, the diagnosed conditions at issue, and the specific causation questions to be addressed. For cases where the causation analysis must address pre-existing conditions, early assembly of the pre-incident medical record is the single most important step in ensuring a complete and defensible opinion.
Causation opinions are available as written record review reports without in-person examination, or in conjunction with an independent medical evaluation when current clinical status is relevant to the causation determination. For cases also requiring medical necessity analysis or future care projections, see the medical necessity review and future medical care review service pages. For matters where the scope is limited to a physician-level review of the medical record without a causation opinion — such as treatment adequacy review or initial case assessment — see the medical record review service. Dr. Dardashti provides causation opinions for plaintiff and defense counsel, insurance carriers, mediators, and courts in California and nationwide.
Related Services & Expertise
Independent Medical Evaluation
Structured examination and written opinion with or without causation analysis.
Future Medical Care Review
Evidence-based projection of future treatment costs once causation is established.
Medical Necessity Review
Clinical necessity analysis for each treatment item once the causal basis is confirmed.
Standard of Care Analysis
Evaluating whether treatment was performed in conformity with accepted clinical practice.
CRPS Expert Witness
Causation, diagnosis, and future care for Complex Regional Pain Syndrome.
Post-Laminectomy Syndrome
Causation analysis for persistent spinal pain following decompression or fusion surgery.
FAQ
Causation Analysis — Common Attorney Questions
- A causation analysis addresses whether a diagnosed medical condition is causally related to a specific event — typically an accident, workplace incident, or medical procedure. In pain management, this includes evaluating whether spinal injuries, neuropathic pain conditions, or diagnoses like CRPS were caused or substantially contributed to by the subject incident, as distinct from pre-existing disease or unrelated factors. The analysis must address not just the temporal relationship between the event and the onset of symptoms, but the biological plausibility, the mechanism of injury, the medical record chronology, and the patient's pre-incident baseline.
- "But-for" causation asks whether the injury would have occurred absent the defendant's conduct. "Substantial factor" causation — the standard more commonly applied in California personal injury litigation — asks whether the defendant's conduct was a material contributing cause, even if not the sole cause. A claimant with pre-existing degenerative disc disease can still establish causation if the subject incident substantially contributed to a new or aggravated condition, even if the degenerative changes were present before the accident. Dr. Dardashti structures causation opinions to align with the applicable legal standard in the jurisdiction, and addresses how the pre-incident baseline and the incident each contributed to the current condition.
- Pre-existing degenerative conditions are common in pain management litigation. A causation opinion must distinguish between underlying disease present before the incident and new or aggravated pathology caused or accelerated by the event. Dr. Dardashti evaluates the claimant's pre-incident medical history, the documented findings before and after the incident, the nature of the pre-existing pathology, and the temporal relationship between the event and the change in clinical status. The opinion addresses whether the subject incident produced a material change — a new symptom pattern, a worsened functional deficit, or a clinical escalation that would not have occurred on the same timeline absent the incident.
- No. An IME includes a physical examination of the claimant; a causation analysis is typically a records-based review that produces a written opinion without an in-person examination. In some cases, both are appropriate: the IME to evaluate current clinical status, and the causation analysis to address the relationship between the incident and the diagnosed condition. Dr. Dardashti can perform either or both depending on case requirements. For cases where the claimant's current clinical presentation is central to the causation question — for example, a disputed CRPS diagnosis where active physical findings are required — an IME may be necessary to complete the causation analysis.
- A complete causation analysis requires medical records from before and after the subject incident, diagnostic imaging reports, treating physician notes, operative and procedure records, and a description of the mechanism of injury. Employment records, prior claim history, and deposition transcripts from treating physicians are also useful. The pre-incident record is as important as the post-incident record — the causation analysis depends on characterizing the medical baseline before the event. Gaps in the pre-incident record are themselves a factor: the absence of documented prior symptoms is relevant to whether the onset of symptoms after the incident represents a new condition rather than a continuation of pre-existing disease.
- Yes. Causation analysis frequently intersects with treatment necessity — for example, whether a lumbar fusion was causally related to a work injury rather than pre-existing degeneration, or whether a spinal cord stimulator implant is an appropriate response to a post-traumatic pain condition. Dr. Dardashti can address both the causal relationship and the medical necessity of the intervention in a single opinion. In many cases, the causation and necessity analyses are inseparable: establishing that the intervention was causally necessitated by the incident requires both that the incident caused the condition and that the condition clinically warranted the intervention.
- Yes. The aggravation doctrine applies to pre-existing conditions that were asymptomatic before the incident as well as to those that were already producing symptoms. A claimant who had degenerative disc disease documented on prior imaging but no documented history of back pain can still establish that an accident aggravated that condition into a symptomatic, functionally limiting state. The key analytical elements are: documenting the absence of prior symptoms through the medical record; establishing the biological plausibility of the aggravation mechanism; and demonstrating that the post-incident clinical course reflects a new symptomatic condition rather than the natural progression of underlying disease.
- No. A normal MRI does not exclude causation for pain conditions that are not reliably imaged. CRPS, myofascial pain, ligamentous injury, peripheral nerve injury at levels below MRI resolution, and early disc injury may all produce clinically significant pain with a normal or near-normal MRI. Conversely, a positive MRI finding must be correlated with the clinical presentation — imaging abnormalities are common in the general population and must be distinguished from incidental findings that predated the incident. The causation analysis evaluates whether the imaging findings, taken together with the clinical presentation, mechanism of injury, and medical history, are consistent with the claimed causal relationship.
- Yes, in certain circumstances. Delayed onset of pain after a traumatic event — particularly in the 24-72 hour window following motor vehicle accidents, soft tissue injury, or surgical procedures — is biologically consistent with the physiology of inflammation and post-traumatic pain sensitization. A claimant who did not report pain immediately after an accident but developed symptoms within days or weeks is not automatically excluded from establishing causation. However, the longer the interval between the incident and the onset of symptoms, the more the alternative explanations must be addressed. The expert must explain the biological mechanism by which the incident could produce delayed symptoms and distinguish the claimed causal chain from a temporal coincidence.
- Multiple-incident cases require the causation analysis to apportion each component of the current condition among the contributing events. The analysis examines: what was the claimant's status after the first incident and before the second; what new injury or worsening did each subsequent incident produce; and what portion of the current clinical picture is attributable to each event versus to the natural progression of the underlying condition. In cases involving serial accidents — for example, a prior motor vehicle accident followed by a workplace injury to the same spinal region — the expert must address each causal link separately while providing a coherent account of the cumulative picture. Apportionment between multiple incidents is one of the most challenging aspects of causation analysis and requires careful record chronology.
- Gaps in treatment — periods when the claimant did not seek or receive medical care — are a common defense challenge to causation. The defense argument is that a claimant who was not receiving treatment during a particular period was not experiencing symptoms serious enough to require care, suggesting either that the condition had resolved or that the prior treatment was not related to the incident. The causation expert addresses whether the gap is clinically consistent with the claimed condition — some pain conditions fluctuate and may not require continuous treatment; others involve barriers to care (insurance lapses, geographic access, financial constraints) that explain the gap without undermining the causal claim. The analysis must distinguish between a gap that reflects recovery and a gap that reflects the non-continuous nature of episodic or intermittent treatment.
- Minor impact claims — particularly low-speed rear-end collisions where vehicle damage is minimal — are among the most frequently contested causation issues in personal injury litigation. The defense position is that a collision producing minimal vehicle damage cannot produce significant soft tissue or spinal injury. The plaintiff position is that biomechanical forces are not reliably predicted by visible vehicle damage, that seat geometry, crash direction, and occupant position affect force transmission in ways not captured by damage estimates, and that pre-existing spinal vulnerability may amplify injury from forces that would be subclinical in a healthier spine. The causation expert must engage the biomechanical literature directly, address the specific collision parameters, and explain whether the documented injuries are biologically consistent with the claimed mechanism given the available evidence.
- These terms are often used interchangeably but carry distinct analytical meanings. An aggravation is a worsening of a pre-existing condition — the condition becomes more symptomatic, more severe, or more functionally limiting as a result of the incident, but the underlying pathology was already present. Acceleration refers specifically to a condition that would have reached its current state eventually through the natural progression of underlying disease, but has reached it earlier than it would have absent the incident. Both aggravation and acceleration are compensable under California's substantial factor causation standard. The distinction matters for damages: an aggravation claim asserts that the condition is now more severe than it would otherwise have been; an acceleration claim asserts that the claimant has reached a deteriorated state earlier than would have occurred without the incident.
- Yes. Complex Regional Pain Syndrome (CRPS) can be causally related to a traumatic event, a surgical procedure, or even a minor injury such as a fracture, soft tissue injury, or peripheral nerve trauma. The causation analysis for CRPS addresses: whether the Budapest Criteria are satisfied — confirming the diagnosis before addressing its cause; whether the triggering event is consistent with the known mechanisms of CRPS onset (trauma, surgical procedure, immobilization, nerve injury); whether the temporal relationship between the event and the onset of CRPS features is consistent with the published literature on CRPS development; and whether alternative explanations for the symptom complex — including factitious disorder, malingering, and other neuropathic conditions — have been adequately evaluated. CRPS causation is among the most contested areas in pain management litigation.
- Causation establishes the scope of recoverable future medical care. Treatment that is causally attributable to the subject incident is compensable as future damages; treatment for conditions unrelated to the incident or for the natural progression of pre-existing disease that would have been required regardless of the accident is not. In practice, the causation analysis must be completed — or at least substantially advanced — before future care projections can be properly scoped. A future care plan that includes treatment for conditions only partially attributable to the incident overstates the damages; one that excludes treatment necessitated by the incident understates them. For cases involving high-cost future care such as spinal cord stimulation or long-term intrathecal therapy, the causation foundation for each projected treatment item must be explicitly addressed in the expert opinion.
Request a Causation Analysis Opinion
Contact Expert Medical Services LLC with your case summary and records. Causation opinions are available with or without in-person examination.