Nationwide Pain & Injury Medical Expert Witness
Future Medical Care Review & Analysis
Evidence-based projection of future medical treatment and associated costs for chronic pain conditions. Structured for use in personal injury damages calculations, settlement negotiations, and trial. Plaintiff and defense.
Request AvailabilityCredentials & Qualifications
- Service
- Future Medical Care Review & Analysis
- Specialty
- Pain Management & Anesthesiology
- Methodology
- Evidence-Based, Published Cost Data
- Report Format
- Written Projection with Supporting Rationale
- Available For
- Plaintiff & Defense
- Conditions
- Chronic Pain, CRPS, Spinal, SCS
What Is Future Medical Care?
Future medical care refers to the treatment a claimant will require going forward as a direct result of a documented injury or condition — including medications, office visits, interventional procedures, implanted devices, rehabilitation services, and psychological support. In personal injury and catastrophic injury litigation, future medical care is a recoverable item of damages. But the claimed amount must be supported by competent medical evidence, not speculation about what treatment the claimant might want or what the maximum possible care would cost.
Future care projections have direct significance for case valuation at every stage of litigation. At the pleadings stage, a credible future care projection establishes the upper range of the plaintiff's damages claim. At mediation, the defensibility of the projection determines how much leverage it provides in settlement negotiations. At trial, the projection is subject to expert cross-examination on the clinical basis for each line item, the published frequency and duration parameters for each procedure, and the cost data applied to each treatment category. A projection that cannot withstand this scrutiny will be dismantled by a prepared defense expert. Where objective functional evidence also underpins non-economic damages claims, the same clinical documentation serves both purposes — for the evidentiary framework connecting objective pain findings to pain and suffering in Texas, see the Gregory v. Chohan pain and suffering damages guide.
Future care projections are most frequently challenged on three grounds: that the projected treatment is not medically necessary for the documented diagnosis; that the projected frequency or duration exceeds what published guidelines support; or that the costs applied exceed what the procedure actually costs in the relevant geographic market. All three challenges can be addressed — but only if the projection was built from the ground up on a medical necessity foundation, guideline-based frequency parameters, and current regional cost data.
How Pain Management Experts Evaluate Future Medical Care
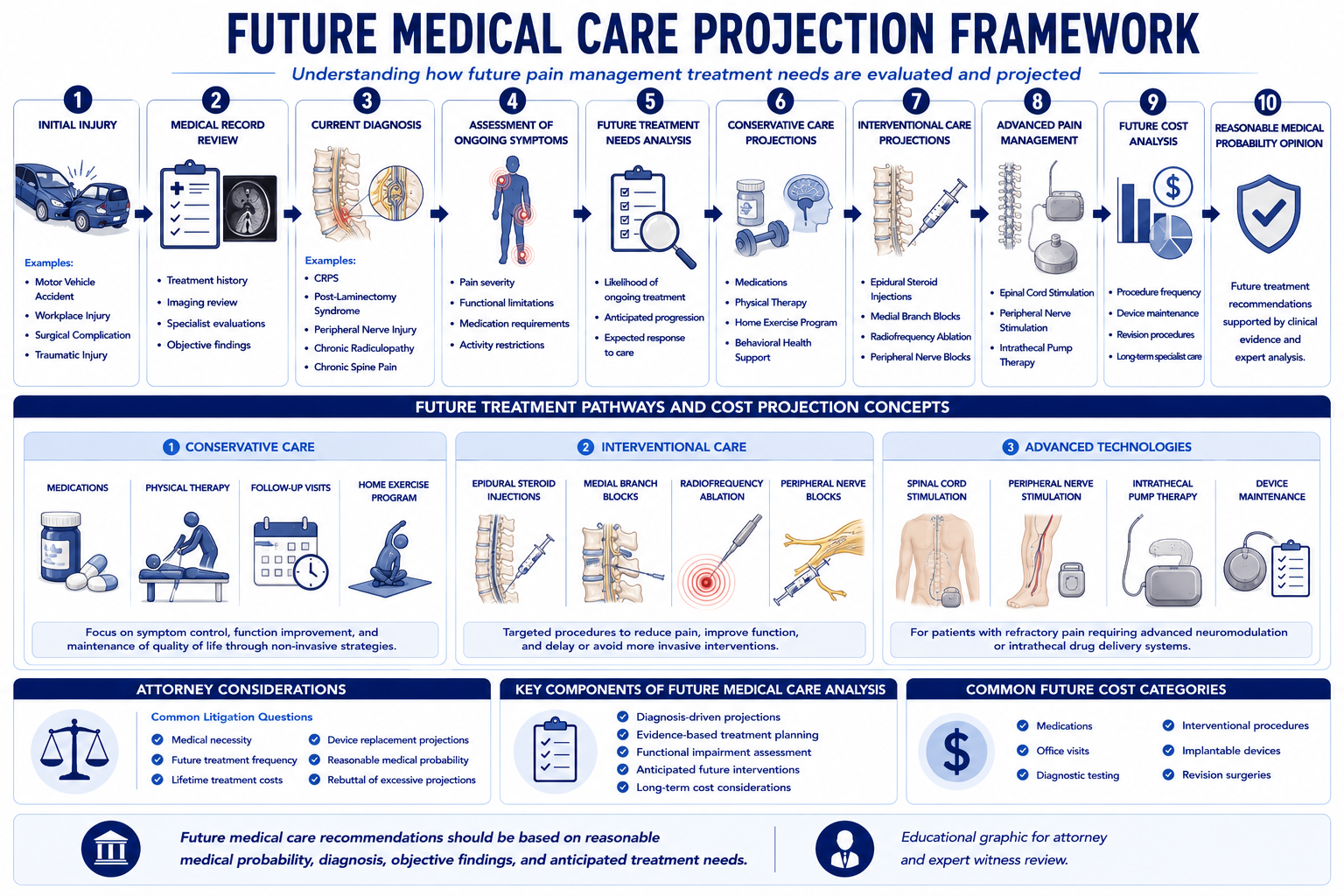
A defensible future care projection is a structured analytical process, not a list of treatments appended to a diagnosis. The following framework governs how Dr. Dardashti approaches every future care engagement.
Current Diagnosis
The projection begins with a confirmed, documented diagnosis. A future care projection for a diagnosis that is not well-supported in the clinical record — or for conditions that are alleged but not confirmed by examination and imaging — is vulnerable to challenge from the first line. The diagnostic foundation must be specific: not "chronic pain" but the specific diagnosed condition, the anatomical level, the mechanism, and the objective findings that confirm it. Each projected treatment item is linked to a specific diagnosis and a specific clinical indication.
Response to Prior Treatment
The most reliable predictor of future treatment is the documented response to prior treatment. A claimant who has received three rounds of epidural steroid injections with documented benefit and then relapsed provides a clear clinical basis for projecting future injection cycles at the guideline-based frequency. A claimant who underwent spinal cord stimulator implantation with documented ≥50% pain reduction and functional improvement provides the clinical foundation for projecting ongoing SCS management, battery replacement, and follow-up programming. The projection must be consistent with the treating record — not more optimistic, not more pessimistic.
Functional Limitations
Functional limitations document the clinical severity of the condition and the treatment requirements that follow from that severity. A claimant with documented inability to ambulate beyond one block, significant activities-of-daily-living limitations, and work incapacity presents a different future care picture than one with mild functional impairment managed conservatively. The functional assessment also informs the duration of treatment — conditions producing severe functional limitation are more likely to require indefinite ongoing management than those with mild functional impact on a trajectory toward resolution. For the clinical methodology used to assess and document functional impairment across examination, validated instruments, and imaging correlation, see the article on how pain management experts objectively evaluate pain.
Imaging Findings
Imaging findings establish the structural basis for the projected treatment. Multi-level degenerative disc disease at the levels treated with epidural injections supports a projection of ongoing injection cycles; severe foraminal stenosis at an instrumented level supports monitoring and possible revision; a post-surgical MRI showing epidural fibrosis and persistent nerve root compression supports a projection that includes escalation to neuromodulation if conservative management is inadequate. Where imaging is inconsistent with the claimed diagnosis or projects an expected improvement over time, the projection must account for the expected clinical trajectory.
Natural History of the Condition
The natural history of the specific diagnosed condition shapes the time horizon and treatment intensity of the projection. Conditions with known progression trajectories — degenerative disc disease, CRPS, post-laminectomy syndrome — require the expert to address whether the condition is stable, slowly progressive, or likely to escalate, and what treatment changes each trajectory implies. A projection that applies a flat treatment rate indefinitely without engaging the known natural history of the condition will be challenged for failing to account for the expected clinical course. When pre-existing degeneration is present, the projection must distinguish future care attributable to the incident from care the claimant would have required from natural disease progression — the methodology for which is addressed in the article on pre-existing degeneration vs. aggravation in spine injury cases.
Treatment Durability
Treatment durability addresses how long each projected intervention is expected to provide benefit and when it will need to be repeated or replaced. For interventional procedures — epidural steroid injections, medial branch blocks, radiofrequency ablation — the published evidence base establishes the typical duration of benefit and the clinical criteria for retreatment. For implanted devices, the manufacturer's published longevity data and the published device revision rates establish when replacement is expected. The projection must use the correct longevity data for the specific device technology and the specific stimulation protocol — not a generic estimate that may overstate or understate the replacement burden.
Risk-Benefit Analysis for Projected Interventions
High-cost projected interventions require an explicit risk-benefit analysis in the future care opinion. For a projection of future SCS surgery, intrathecal pump implantation, or repeat major spinal surgery, the expert must address: whether the documented clinical trajectory supports the projected intervention; whether the patient's comorbidities are consistent with undergoing the procedure safely at the projected age; and whether the expected benefit justifies the procedural risk at the projected point in the clinical trajectory. A projection that includes major surgical procedures for a patient whose age and comorbidity burden at the time of projected surgery would make them a marginal surgical candidate is vulnerable to challenge on risk-benefit grounds.
Future Medical Care by Condition
The structure and scope of a future care projection varies substantially by the specific pain condition at issue. Each condition has a known natural history, a characteristic treatment trajectory, and a set of published guidelines that govern what care is expected and at what frequency.
Complex Regional Pain Syndrome
CRPS is one of the most expensive and complex chronic pain conditions to project because of the breadth of treatment it may require across its clinical trajectory. A complete CRPS future care projection addresses: pharmacological management (membrane stabilizers, sympatholytic agents, low-dose naltrexone, topical agents); interventional treatment (sympathetic nerve blocks, stellate ganglion blocks, lumbar sympathetic blocks); physical and occupational therapy for desensitization and functional restoration; psychological support given the well-documented role of central sensitization and psychological comorbidity; and potential escalation to spinal cord stimulation or peripheral nerve stimulation if conservative management is insufficient. CRPS projections require a longer time horizon and more scenario-based analysis than most pain conditions because the clinical course is less predictable. For the full CRPS litigation framework, see the CRPS expert witness guide.
Post-Laminectomy Syndrome
Post-laminectomy syndrome — persistent spinal pain following decompression or fusion surgery — is one of the most common and most litigated chronic pain conditions, with a well-established treatment trajectory that makes future care projections more predictable than for conditions with less published natural history data. The standard future care projection for post-laminectomy syndrome includes: ongoing interventional management (epidural steroid injections, medial branch blocks, and radiofrequency ablation cycles at the affected levels); potential escalation to spinal cord stimulation if the interventional trajectory is insufficient; long-term pharmacological management; and physical therapy for functional maintenance. The projection must address the known escalation pattern — from injections to neuromodulation — and explain why the specific patient's clinical status at the time of projection supports or does not yet require the higher-cost interventional modalities.
Peripheral Nerve Injury
Peripheral nerve injury future care projections address the specific nerve affected, the severity of injury (neurapraxia, axonotmesis, neurotmesis), the expected recovery trajectory, and the treatment required to manage residual neuropathic pain. For incomplete recovery cases, the projection includes: ongoing pharmacological management for neuropathic pain; possible peripheral nerve stimulation if the nerve is amenable to stimulation; and interventional management for associated pain generators. For cases involving complete denervation with expected permanent neuropathic pain, the projection must account for the full duration of the claimant's expected survival.
Chronic Radiculopathy
Chronic radiculopathy — persistent nerve root pain from disc herniation, foraminal stenosis, or post-surgical scar tissue — has a characteristic treatment trajectory of serial epidural steroid injection cycles, with potential escalation to surgical revision or spinal cord stimulation in refractory cases. The future care projection must address: the frequency and duration of injection cycles supported by the prior treatment response; the expected interval between injection series; the medical necessity of spinal cord stimulation if the injection trajectory is insufficient; and the escalation criteria that would trigger consideration of surgical revision. Projections that assume indefinite injection series at the maximum guideline frequency without considering the expected clinical trajectory overstate the damages in most chronic radiculopathy cases.
Amputation and Phantom Limb Pain
Amputation and phantom limb pain future care projections are among the most complex because of the multi-modal nature of post-amputation pain management and the long time horizons involved in cases of traumatic limb loss. The projection must address: pharmacological management for phantom limb pain (membrane stabilizers, NMDA antagonists, opioid management where indicated); neuromodulation options including spinal cord stimulation and peripheral nerve stimulation where applicable; mirror therapy and graded motor imagery as non-pharmacological components; and the interface of the pain management plan with the prosthetics and rehabilitation components typically projected in catastrophic injury life care plans. The pain management projection must be coordinated with — and not duplicative of — the other life care plan components.
Future Medical Care by Procedure
Each interventional procedure in pain management has characteristic frequency parameters, expected longevity, known revision risk, and cost structure that governs how it is projected in future care disputes.
Epidural Steroid Injections
Epidural steroid injections (ESIs) are typically projected as recurring series at intervals determined by the documented response to prior injections. Published guidelines generally limit ESIs to three to four injections per spinal region per year, with the specific frequency depending on the clinical indication and prior response documentation. The projection must specify the approach (interlaminar, transforaminal, or caudal), the level and laterality, and the basis for the projected frequency. Cost includes the facility fee, physician fee, fluoroscopic guidance, and contrast. Defense experts frequently challenge projections that apply the maximum guideline frequency indefinitely without clinical justification.
Medial Branch Blocks and Radiofrequency Ablation
Medial branch block and radiofrequency ablation (RFA) are projected as a diagnostic-therapeutic sequence. The projection must account for: the diagnostic block series required before each RFA cycle (typically two blocks); the RFA procedure at the confirmed levels; and the expected re-denervation interval before the ablation effect wanes and the cycle repeats. The re-denervation interval is individual and depends on nerve regeneration — the projection must be grounded in the prior documented response duration, not a generic interval. Cost includes each diagnostic block, the RFA facility and physician fees, and fluoroscopic guidance. Future care projections for RFA that do not include the required diagnostic block cycle before each ablation understate the actual cost of the treatment sequence.
Spinal Cord Stimulation
Spinal cord stimulation (SCS) future care projections require the most granular device-specific analysis of any pain management procedure because of the high implant cost, the device replacement cycle, and the ongoing programming and follow-up requirements. The projection must address: the trial phase (percutaneous lead trial costs, explant or conversion costs); the permanent implant (implant surgery, hardware, facility); ongoing follow-up programming visits; battery replacement at the manufacturer-specified interval for the specific device technology; and the published risk of lead revision. For rechargeable devices, the battery life is substantially longer than for primary cell devices, and the projection must apply the correct interval. The article on how pain management experts evaluate medical necessity for spinal cord stimulators addresses the necessity foundation required before SCS can be projected as future care.
Intrathecal Pump Therapy
Intrathecal pump therapy (ITP) future care projections are among the most cost-intensive in pain management because they involve an initial high-cost surgical implant, recurring drug refill visits, catheter maintenance, and scheduled pump replacement at manufacturer-specified intervals (typically 5–7 years for current-generation devices). The projection must address: the intrathecal drug trial (outpatient or inpatient); the permanent implant surgery and hardware; refill visits at the clinically appropriate interval (monthly to quarterly depending on reservoir size and drug consumption); and scheduled pump replacement over the projection period. Drug costs are a significant component of ITP projections and must reflect current compounded drug pricing or commercial drug costs depending on the formulation used.
Peripheral Nerve Stimulation
Peripheral nerve stimulation future care projections follow the same general structure as SCS — trial phase, permanent implant, follow-up, and device replacement — but with device-specific longevity data for PNS systems, which differ from SCS device longevity. PNS projections must address the specific nerve target, the documented trial response, and the published evidence base for the specific PNS application, which is less mature than for SCS and may require explicit engagement with the literature supporting the projected indication.
Opioid and Non-Opioid Medication Management
Long-term pharmacological management projections must address: the specific medications projected and their clinical basis; the dose and frequency consistent with published guidelines; the monitoring visits required for long-term opioid therapy (urine drug screening, PDMP queries, functional assessment); and the projected duration grounded in the natural history of the condition and the established treatment trajectory. Defense experts challenge long-term opioid projections on medical necessity and CDC guideline compliance grounds; projections that engage the guideline literature directly and explain why the specific patient's condition supports long-term pharmacological management are more defensible than those that project maximum doses indefinitely.
Common Disputes Regarding Future Medical Care
The following dispute patterns arise most frequently in future medical care expert disagreements. Understanding each pattern allows attorneys to evaluate their projection's exposure before producing it in discovery.
- Overprojection: A future care projection that includes treatment modalities not indicated for the documented diagnosis, procedures at frequencies exceeding published guideline limits, or costs applied at rates above market benchmarks. Overprojection is the most common defense challenge and is most effective when the opposing expert can point to specific guideline provisions that cap the frequency or duration of the projected treatment. The defense argument is not merely that the total is too high — it is that specific line items are unsupported and would not be ordered by a competent treating physician.
- Underprojection: A defense-sponsored future care projection that excludes clinically indicated treatment, applies costs below market rates, or projects an unrealistically short duration of care for a condition with a known long-term treatment trajectory. Defense projections that omit expected SCS battery replacement, underestimate injection cycle frequency, or apply costs from geographic markets significantly less expensive than the claimant's treating region understate the actual future care burden.
- Unsupported life care plans: A life care plan that projects expensive treatment without a physician opinion supporting the medical necessity of each treatment item. Defense experts will challenge specific life care plan items by identifying the absence of a clinical foundation — no treating physician who has recommended the projected treatment, no published guideline supporting the projected indication. A life care plan supported by a physician expert opinion on each major treatment category is significantly more defensible than one assembled from literature alone.
- SCS replacement assumptions: The most frequently challenged device-specific projection issue. Defense experts challenge SCS battery replacement projections that apply primary-cell replacement intervals to rechargeable devices, that use outdated device longevity data, or that fail to account for the specific stimulation programming the patient is using. The projection must identify the specific device implanted and apply the manufacturer's published longevity data for that device and stimulation protocol.
- Revision surgery assumptions: Future projections of revision surgery — SCS revision, ITP catheter revision, or spinal surgical revision — must be grounded in the published revision rates for the condition and the specific clinical trajectory of the patient. A projection that assumes revision surgery without documenting the clinical basis for expecting revision overstates the damages; one that omits expected revision in a patient with documented lead instability or progressive hardware failure understates them.
- Long-term opioid management assumptions: Projections of indefinite high-dose opioid therapy for chronic non-cancer pain are among the most challenged future care items. The CDC prescribing guideline, the state medical board guidance, and the published evidence base for long-term opioid therapy all impose requirements that must be addressed in the projection. A projection that assumes indefinite high-dose opioids without engaging these guidelines will be challenged by defense experts who can demonstrate that the projected treatment plan is inconsistent with the applicable prescribing standard.
Plaintiff and Defense Perspectives
Plaintiff Position
Plaintiff future care experts establish the full scope of clinically indicated treatment — the most probable course of care the claimant will require for the documented condition over the applicable time horizon. The core elements of a strong plaintiff future care opinion are: a confirmed, well-documented diagnosis that supports each projected treatment modality; documented prior treatment response that grounds the projected frequency; guideline-based frequency and duration parameters that protect the projection from challenge; current regional cost data from published sources; and a time horizon grounded in the natural history of the condition and the claimant's life expectancy.
Plaintiff future care opinions are strongest when they are conservative enough to withstand challenge while comprehensive enough to capture the full expected treatment burden. A projection that includes every possible treatment modality at the maximum possible frequency is vulnerable to attack and may reduce the jury's confidence in the entire opinion. A projection that is grounded, line by line, in the clinical record and published guidelines survives cross-examination and provides a more credible and ultimately more valuable damages foundation.
Defense Position
Defense future care experts identify specific overstatements in the plaintiff's projection — line items that exceed published guideline parameters, procedures projected without adequate medical necessity foundation, device replacement intervals that are inconsistent with the specific device technology, or cost data applied at rates above the applicable market. The most effective defense challenges are specific and record-grounded: not "the total is too high" but "this specific projected item is not supported by the published indication criteria for this diagnosis."
Defense experts also evaluate whether the causation analysis underlying the projection is complete — whether each projected treatment item is grounded in a condition that is causally attributable to the incident rather than in the natural progression of pre-existing disease. A future care projection that includes treatment for conditions partially attributable to the incident and partially attributable to pre-existing disease requires careful apportionment, and defense experts will identify any failure to apportion as an overstatement of the incident-attributable damages.
Rebuttal Methodology
Effective rebuttal of an opposing future care opinion identifies the specific clinical arguments that are inconsistent with the published evidence base, the documented treating record, or the applicable guideline standard. Rebuttal does not simply reassert the original projection — it engages the opposing expert's specific arguments and demonstrates where those arguments are inconsistent with the full record or with the published literature the opposing expert applied or failed to apply. Rebuttal opinions are available as supplemental declarations, written reports, or deposition testimony following review of the opposing expert's written opinion.
Future Medical Care and Causation
Causation establishes which conditions are attributable to the subject incident — and only conditions attributable to the incident are compensable as future care damages. Treatment for conditions that would have been required regardless of the incident, or that are attributable to the natural progression of pre-existing disease, is not recoverable from the defendant. The future care projection must therefore be preceded by a causation analysis that identifies the incident-attributable conditions and distinguishes them from conditions that were present or would have developed regardless.
In aggravation cases — where the incident worsened a pre-existing condition — the future care projection must address the incremental treatment burden attributable to the aggravation. Treatment that the claimant would have required for the pre-existing condition regardless of the incident is not included; treatment required at greater intensity, greater frequency, or sooner than the natural history would have produced is included as incident-attributable future care. For California-specific discussion of how this analysis applies in personal injury litigation, see the California pain management expert witness guide.
In cases involving subsequent accidents or multiple incidents, each contributing event's share of the future care burden must be addressed. The projection cannot simply attribute all future care to the incident at issue without accounting for the contribution of other events to the current clinical state. The causation analysis must be structured to support this apportionment, and the future care projection must be consistent with the causation conclusion.
Future Medical Care and Medical Necessity
Every line item in a future care projection rests on a medical necessity determination. A projected future treatment that cannot survive a necessity challenge at deposition should not appear in the projection. The medical necessity analysis provides the clinical foundation for each projected item — linking the proposed treatment to a documented diagnosis, a published clinical indication, a guideline-based frequency, and the treating record demonstrating a clinical trajectory that supports the projection.
For high-cost future interventions, the necessity analysis is particularly critical. A projection of future SCS implantation requires: documentation that the underlying condition meets published SCS indications; documentation that conservative and interventional treatments preceding SCS have been trialed; and, if the claimant has not yet undergone SCS, a clinical rationale for why the trajectory supports SCS at the projected point in the future care plan. A projection that assumes SCS without addressing the medical necessity of neuromodulation for the specific condition will be challenged on necessity grounds before the cost question is even reached.
The relationship between future care and necessity also governs duration. A projected treatment that is medically necessary at one point in the clinical trajectory may not be medically necessary indefinitely — the projection must engage the question of when ongoing treatment would be expected to cease (if the condition is expected to resolve), when it would be expected to escalate (if the natural history supports progression), and what the applicable guideline parameters say about the appropriate duration of each projected modality.
Documentation Required for Future Care Review
The following records are required for a complete and defensible future care analysis:
- Complete treating record: All treating physician notes, procedure records, and diagnostic imaging from the post-incident period, covering the full treatment trajectory to date.
- Current treatment status: The most recent treating physician notes and any records from the three to six months preceding the expert engagement, establishing the current clinical baseline from which future care is projected.
- Prior treatment response documentation: Records documenting what treatment has been rendered and the patient's documented response — pain score changes, functional assessment, and physician assessment of treatment benefit at each stage.
- Device records: For SCS, ITP, and PNS cases — device specification sheets, implant records, programming visit notes, and battery interrogation records that establish what device is implanted and at what stimulation parameters it is operating.
- Prior future care projections: Any life care plans or future care projections previously produced in the case, for comparison and potential rebuttal.
- Causation analysis: A completed or concurrent causation analysis establishing which conditions are attributable to the incident and should be addressed in the future care projection.
- IME or current clinical examination: An independent examination of current clinical status is valuable when the most recent treating records are more than six months old or when current functional status is directly relevant to the scope of future care projected.
How to Request a Future Medical Care Review
Contact Expert Medical Services LLC with the case records, the diagnosed conditions to be addressed, and the specific future care questions to be answered. For cases requiring causation analysis before the future care projection can be scoped, a concurrent or sequential causation analysis can be initiated in the same engagement. For cases also requiring an in-person examination to assess current clinical status, an independent medical evaluation can be combined with the future care review. For cases involving a disputed life care plan or a defense challenge to specific future care items, the engagement can be structured as a rebuttal opinion focused on the specific items in dispute.
Future medical care opinions are available as written projections, supplemental declarations responding to opposing future care opinions, and deposition or trial testimony. Dr. Dardashti provides opinions for plaintiff and defense counsel, insurance carriers, life care planners seeking physician support, mediators, and courts in California and nationwide. For cases requiring both medical necessity review and future care projection — particularly high-cost device-based cases — both analyses can be structured as a coordinated engagement with consistent clinical findings across both opinions.
Related Services & Expertise
Causation Analysis
Establishing the causal basis before projecting future medical needs.
Medical Necessity Review
Clinical necessity analysis for each projected treatment item.
Independent Medical Evaluation
Structured examination of current clinical status — foundation for future care projection.
Spinal Cord Stimulation
SCS cost analysis, device longevity, and medical necessity in future care disputes.
CRPS Expert Witness
Future care projections for Complex Regional Pain Syndrome — one of the most complex chronic pain conditions to project.
Intrathecal Pump Therapy
ITP future care including drug refills, catheter maintenance, and pump replacement cycles.
FAQ
Future Medical Care — Common Attorney Questions
- A future medical care review is a physician's analysis of the medical treatment a claimant will require as a result of a documented injury or condition, and the associated costs over the relevant time period. In personal injury cases, future medical care is a component of damages. A pain management physician is qualified to project future care for chronic pain conditions, interventional procedures, and long-term medication management. The projection must be grounded in the documented diagnosis, the published clinical guidelines for the condition, and the treating record — not in speculation about what treatment the claimant might want or might receive.
- Future medical cost projections are based on the documented diagnosis, the evidence-based treatment protocols for that condition, the claimant's age and expected remaining years of treatment, and published cost data for the applicable geographic market. For pain management, this may include medication costs, office visits, interventional procedures (injections, nerve blocks, ablation), psychological support, physical therapy, and durable medical equipment. Where a device such as a spinal cord stimulator or intrathecal pump is indicated, device costs, implantation, ongoing follow-up, and scheduled replacement are addressed separately. The projection must be specific enough to survive cross-examination on both the clinical basis for each projected item and the cost data applied.
- A life care plan is a comprehensive, multi-disciplinary document addressing all future needs — medical, functional, equipment, and sometimes vocational — typically prepared by a certified life care planner in catastrophic injury cases. A future medical care projection is a physician's opinion on the medical treatment specifically required for a diagnosed condition, often narrower in scope and produced by the treating or consulting physician. In litigation, both may be used; they serve different but complementary evidentiary functions. A life care planner quantifies needs across multiple domains; the physician expert provides the clinical foundation for the medical treatment component and can support or rebut specific line items in a life care plan.
- Yes. When a major intervention such as spinal cord stimulation, intrathecal drug delivery, peripheral nerve stimulation, or repeat surgery is projected as future care, the opinion must address: whether the intervention is medically indicated given the diagnosis and prior treatment history; what the expected costs are for the trial period and permanent implant; what ongoing costs — device maintenance, battery replacement, follow-up programming — are attributable to the condition over the relevant timeframe; and what the published longevity data show for the specific device. A projection that includes SCS without addressing the medical necessity of neuromodulation for the specific documented condition will not withstand expert challenge at deposition.
- Yes. Defense attorneys frequently retain a pain management physician to evaluate whether the claimant's proposed future care is medically necessary, appropriately scoped, and accurately priced. A defense-side future care review may identify treatment that exceeds what the evidence supports for the documented condition, procedures that are not indicated under published guidelines, cost estimates that exceed published market rates, or projection durations that exceed the expected clinical trajectory. Dr. Dardashti provides these opinions for defense as well as plaintiff counsel.
- A complete set of medical records is required, including treating physician notes, procedure records, diagnostic imaging, pharmacy records, and any prior future care plans or life care plans that have been produced in the case. Current treatment information is important for assessing what care has been established and what additional treatment is projected. For device-based future care — SCS, ITP, PNS — the existing trial and implant records, device programming notes, and device representative records establish the clinical trajectory that supports the projection. An IME examination may also be useful to assess current clinical status before projecting future needs.
- Spinal cord stimulator battery life varies by device technology and stimulation usage. Traditional rechargeable SCS devices have battery replacement intervals of 5–10 years depending on usage parameters; non-rechargeable (primary cell) devices may require more frequent replacement. High-density and burst stimulation programs consume power faster, affecting replacement intervals. The future care projection must address: the specific device type implanted; the published battery longevity data for that device; the clinically expected stimulation parameters based on the patient's condition; and the total replacement cost including surgical replacement, device hardware, and follow-up programming. Defense experts frequently challenge projections that apply non-rechargeable replacement intervals to rechargeable devices, or that project replacement intervals shorter than the published device longevity data support.
- Yes, and they frequently are. A future care projection is speculative — and vulnerable to exclusion or reduction — if it includes treatment for a diagnosis that is not well-supported in the record, projects procedures at frequencies exceeding published guideline limits without clinical rationale, projects device costs without addressing the medical necessity of the specific device for the specific condition, or applies cost data that is not geographically applicable. A defensible projection links each line item to a documented diagnosis, a published clinical indication, a treatment frequency consistent with the guideline literature, and current regional cost data. Projections that survive cross-examination are those that the expert can defend line by line at deposition.
- Revision surgery and device replacement require the same medical necessity foundation as the original procedure. For implanted devices — SCS, ITP, PNS — the published device longevity data establishes when scheduled replacement is expected; the projection must apply the correct replacement interval for the specific device technology and stimulation protocol. For revision surgery — lead revision, pocket revision, or full explant and reimplant — the projection must establish the clinical basis for expecting revision: the published revision rates for the condition at issue, the device-specific complication rates, and the clinical trajectory of the specific patient. A projection that assumes the maximum possible revision rate without clinical justification will be challenged; one grounded in published complication and revision data is more defensible.
- The legally relevant standard for future care damages is the most probable future treatment — what the claimant is more likely than not to require given the documented condition, the published natural history, and the established treatment trajectory. A best-case projection (minimum expected treatment) understates the damages; a worst-case projection (maximum possible treatment) overstates them. Effective future care projections are grounded in the most probable scenario: the treatment that a competent pain management physician would expect to be clinically indicated for this patient's documented condition over the projected time period, based on the published guideline frequency and duration parameters. Deviating from the most-probable standard toward either extreme weakens the opinion at deposition and reduces the jury's confidence in the projection.
- Pre-existing degenerative conditions complicate future care projections in two directions. First, treatment for the pre-existing condition that would have been required regardless of the incident is not compensable as future damages from the incident — the projection must distinguish between incident-related future care and care attributable to the natural progression of pre-existing disease. Second, when the incident has accelerated the progression of a pre-existing condition, the future care projection must address the incremental treatment burden attributable to the incident — the care the claimant will require sooner or at greater intensity than would have been expected from the natural history of the underlying disease. The distinction requires a causation analysis to precede and inform the future care projection.
- Yes, in appropriate cases. Long-term opioid management for documented chronic pain conditions is projectable as future care when: the diagnosis clinically supports ongoing pharmacological management; non-opioid alternatives have been trialed and documented as inadequate; the projected dose and duration are within published guideline parameters; and the necessity of ongoing management is grounded in the natural history of the condition. Defense experts frequently challenge long-term opioid projections on medical necessity and guideline compliance grounds. The projection must engage CDC prescribing guidelines and state medical board guidance and explain why the specific patient's condition supports long-term opioid management rather than dose reduction or transition to alternative modalities.
- Future medical care projections are among the most important quantitative inputs into settlement valuation. A well-grounded projection establishes a defensible damages floor for the plaintiff and forces the defense to justify any reduction with expert support. A projection that is vulnerable to challenge — overstated, poorly grounded, or inconsistent with published guidelines — weakens the plaintiff's settlement position because the defense can demonstrate the vulnerability without needing to go to trial. At mediation, the strength and defensibility of the future care projection is as important as the dollar amount: mediators and experienced defense counsel will evaluate whether the projection can survive cross-examination, not just what it says. A projection structured for trial — with each line item linked to a specific diagnosis, clinical indication, and cost basis — is significantly more effective in settlement discussions than one prepared primarily for impact.
- CRPS is one of the most expensive chronic pain conditions to manage long-term because of the breadth of treatment modalities it may require, the unpredictability of its clinical course, and the potential need for escalation to high-cost neuromodulation. A future care projection for CRPS must address: the projected pharmacological management including sympatholytic agents, membrane stabilizers, and neuropathic agents; the interventional treatment trajectory including sympathetic blocks and possible spinal cord stimulation or peripheral nerve stimulation if conservative management is insufficient; the rehabilitation component including desensitization therapy, physical therapy, and occupational therapy; and psychological support given the documented role of central sensitization and psychological comorbidity in CRPS. CRPS projections require a longer time horizon than most pain conditions and must be grounded in the Budapest-confirmed diagnosis to survive challenge.
- A certified life care planner (CLCP) collects input from multiple treating providers, applies published cost data, and assembles the multi-domain future care plan addressing medical, rehabilitation, equipment, and support needs. A physician expert provides the clinical opinion — the diagnosis-based rationale for each projected treatment modality — that gives the life care plan its medical foundation. A life care planner without a physician foundation is vulnerable to challenge; a physician projecting costs without current cost data is similarly vulnerable. In well-structured cases, the physician expert provides a clinical opinion supporting the medical treatment component, and the life care planner assembles the full plan with current cost data. Dr. Dardashti can serve as the physician foundation for a life care planner's work or can independently project future medical care costs for cases that do not require a full life care plan.
Request a Future Medical Care Analysis
Available for plaintiff and defense. Contact Expert Medical Services LLC with case records and specific conditions to be addressed.