Nationwide Pain & Injury Medical Expert Witness
Peripheral Nerve Stimulation Expert Witness
Expert evaluation of peripheral nerve stimulation medical necessity, trial stimulation documentation, lead migration, device complications, candidate selection, standard of care, causation analysis, and future medical care projections in neuropathic pain, peripheral nerve injury, CRPS Type II, phantom limb pain, and complex injury litigation.
Request AvailabilityCredentials & Qualifications
- Topic
- Peripheral Nerve Stimulation (PNS)
- Also Known As
- Peripheral Nerve Stimulator, Subcutaneous PNS, sPNS
- Specialty
- Pain Management & Neuromodulation
- Evaluation Areas
- Medical Necessity, Causation, Future Care
- Review Scope
- Records Review & IME
- Testimony
- State & Federal Courts
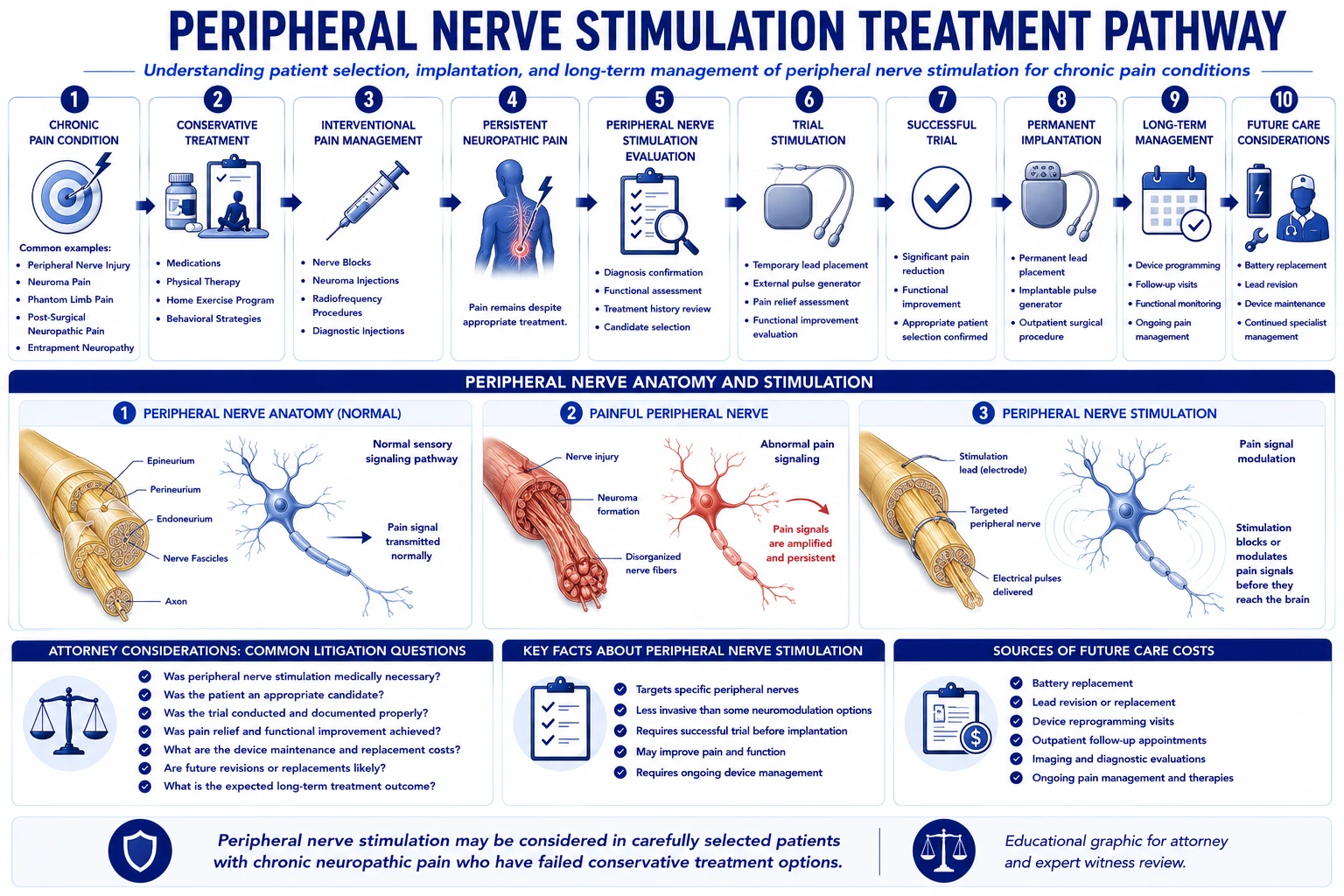
What Is Peripheral Nerve Stimulation?
Peripheral nerve stimulation (PNS) is an implantable neuromodulation procedure in which one or more electrical leads are placed adjacent to a targeted peripheral nerve — outside the spinal canal — and connected to an implantable pulse generator (IPG) that delivers programmable electrical stimulation. The stimulation modulates pain signal transmission at the peripheral nerve level, producing analgesia confined to the distribution of the targeted nerve. Unlike spinal cord stimulation, which targets the dorsal columns for broad segmental coverage across a dermatomal territory, PNS is directed at a discrete named nerve, making it most appropriate when neuropathic pain is localized to the distribution of a specific, identifiable peripheral nerve.
PNS leads may be placed percutaneously — using a needle-based technique under ultrasound or fluoroscopic guidance — or surgically via open exposure of the target nerve, depending on the anatomy of the nerve and the device platform used. The IPG may be non-rechargeable, with a finite battery life requiring periodic surgical replacement, or rechargeable, requiring patient compliance with external charging protocols. Device platform selection affects both the initial implantation approach and the long-term cost structure, making device identification an important element of PNS future care projections.
In the medical-legal context, PNS arises in personal injury damages analysis as proposed future care, and in malpractice matters involving device complications, inappropriate candidate selection, or failures in post-implant management. Expert review addresses the pain management dimensions of these cases — medical necessity, candidacy, trial documentation, device management, and future care — rather than the neurosurgical or device engineering aspects of implantation technique.
Conditions Commonly Treated with PNS
PNS is indicated for refractory neuropathic pain that is anatomically localized to the territory of a specific peripheral nerve and that has failed an adequate trial of conservative pharmacological and interventional management. The conditions most commonly encountered in PNS-related litigation reflect this peripheral nerve-specific profile:
- › Peripheral nerve injury — Direct traumatic, surgical, traction, or compression injury to a named peripheral nerve producing refractory neuropathic pain in the nerve's distribution is the most common substrate for PNS consideration in personal injury litigation. Peripheral nerve injuries from motor vehicle accidents, workplace incidents, and iatrogenic surgical complications are frequent antecedents. Because PNS targets the injured nerve directly, it addresses the pain source at the peripheral level rather than relying on central modulation — which is the clinical rationale for preferring PNS over SCS in discrete nerve injury cases.
- › Neuroma pain — When a peripheral nerve is severely or completely divided, the proximal nerve end may develop a traumatic neuroma — a disorganized mass of regenerating nerve fibers that is exquisitely sensitive to mechanical stimulation and a potent source of spontaneous ectopic discharge. Neuroma pain following amputation, laceration, or surgical nerve sectioning can be refractory to pharmacological management and perineural injection therapy. PNS targeting the proximal nerve segment proximal to the neuroma provides sustained stimulation that may suppress the ectopic discharge underlying neuroma pain. Neuroma formation following surgical procedures introduces iatrogenic causation issues when surgical technique or postoperative management is implicated.
- › Phantom limb pain — Neuropathic pain perceived in the absent portion of an amputated limb arises from maladaptive reorganization of peripheral and central nociceptive pathways following amputation. PNS targeting residual limb nerve ends has reported efficacy in cases refractory to pharmacological management and conventional interventional approaches. In high-value personal injury cases involving traumatic amputation, phantom limb pain and the neuromodulation options for managing it — including PNS — are frequently the subject of future care disputes.
- › CRPS Type II — Complex Regional Pain Syndrome Type II — historically termed causalgia — develops in the distribution of a specific peripheral nerve injury and, unlike CRPS Type I, has a confirmed peripheral nerve substrate. Because CRPS Type II is defined by the presence of a peripheral nerve injury, PNS targeting the involved nerve is a recognized treatment approach for refractory cases. The Type I / Type II distinction has direct implications for PNS candidacy: PNS is more clinically justified in Type II, where an anatomically defined peripheral nerve target exists. Defense review of PNS in CRPS cases may challenge whether the CRPS diagnosis was Type I or Type II, since an undifferentiated CRPS Type I diagnosis does not provide the peripheral nerve substrate necessary to support PNS as the preferred modality.
- › Post-surgical neuropathic pain — Iatrogenic peripheral nerve injury from surgical procedures — including entrapment or traction injuries from retractors, direct nerve division, or scar encasement of peripheral nerves — can produce refractory neuropathic pain in a defined nerve distribution. In malpractice matters where a surgical complication is alleged to have caused peripheral nerve injury and subsequent PNS candidacy, both the causation analysis and the standard of care review for the index surgical procedure are relevant to the overall damages assessment.
Neuromodulation Principles
Peripheral nerve stimulation achieves pain relief through electrical modulation of nociceptive signal transmission at the peripheral nerve level. Understanding the neuromodulatory mechanism is relevant in litigation when questions arise about why a PNS device produced insufficient or unexpected coverage, or when the appropriateness of PNS for the specific clinical presentation is contested.
The foundational mechanism is gate control theory, originally described by Melzack and Wall: activation of large-diameter Aβ mechanosensory fibers by sub-threshold electrical stimulation inhibits transmission of pain signals carried by small-diameter C and Aδ nociceptors at the same spinal segmental level. By creating controlled activation of Aβ fibers in the stimulated peripheral nerve, PNS generates an inhibitory signal that modulates — or "gates" — the ascending pain signal before it reaches the spinal cord dorsal horn. This produces the characteristic paresthesia or sub-threshold stimulation sensation in the nerve's distribution and suppresses ongoing neuropathic pain in that territory.
More recent evidence has expanded the mechanistic picture beyond gate control. Sustained peripheral nerve stimulation produces antidromic and orthodromic effects on peripheral nociceptor sensitization — reducing the abnormal spontaneous discharge characteristic of injured peripheral nerve. Stimulation also reduces local release of nociceptive neuropeptides (substance P, calcitonin gene-related peptide) from peripheral nerve terminals, contributing to diminished neurogenic inflammation in the stimulated distribution. At the central level, sustained peripheral nerve stimulation engages descending inhibitory pathways — including serotonergic and noradrenergic projections from the brainstem — producing a broader analgesic effect that extends beyond the immediate stimulation period.
These mechanistic considerations inform the medical necessity and standard of care analysis in several ways. First, PNS achieves its effect by activating intact Aβ fibers — which requires that the targeted peripheral nerve retain some Aβ fiber complement. In cases of complete peripheral nerve transection with total deafferentation, the mechanistic basis for PNS is weakened. Second, the confinement of the PNS effect to the stimulated nerve's distribution means that accurate nerve targeting is essential to clinical efficacy — incorrect lead placement relative to the target nerve is a technical failure that may explain inadequate coverage. Third, the known mechanisms provide a clinical basis for explaining why PNS may fail or produce incomplete relief in specific anatomical or pathophysiological settings, which is relevant to expert opinion on expected clinical outcomes and future care planning.
PNS vs. Spinal Cord Stimulation
The distinction between peripheral nerve stimulation and spinal cord stimulation is a recurring clinical and standard of care issue in neuromodulation litigation. The two modalities occupy distinct positions in the pain management spectrum, and selecting the appropriate modality for a given clinical presentation is a clinical judgment with direct medical necessity and standard of care implications.
- › Target anatomy — SCS targets the dorsal columns of the spinal cord via epidural leads placed in the spinal canal; PNS targets a discrete peripheral nerve via leads placed adjacent to the nerve outside the spinal canal. The anatomical target difference drives the coverage difference: SCS produces broad segmental coverage across a dermatomal territory; PNS produces coverage confined to the territory of the stimulated nerve.
- › Pain distribution requirements — SCS is generally preferred when pain spans multiple dermatomes, has an axial predominance, or does not correspond to a discrete named nerve distribution. PNS is preferred when pain is anatomically restricted to the territory of a specific, identifiable nerve — such as the sural nerve, saphenous nerve, radial sensory nerve, or the terminal branches of the common peroneal nerve. Attempting to use PNS to cover a multi-dermatomal pain distribution that would require multiple lead placements at multiple separate nerves increases procedural risk and device complexity without the coverage efficiency of a single epidural SCS lead.
- › Spinal anatomy considerations — SCS requires epidural lead placement and is contraindicated or technically challenging in patients with prior multilevel spinal instrumentation, severe spinal stenosis at the target level, or spinal anatomy that precludes epidural access. PNS, operating entirely outside the spinal canal, avoids these constraints and may be the preferred neuromodulation option when spinal anatomy makes SCS impractical. Conversely, PNS is limited by the accessibility and anatomy of the target peripheral nerve — nerves in anatomically complex locations or immediately adjacent to major vascular structures require careful approach planning.
- › Sequential and complementary use — PNS and SCS are not mutually exclusive. A patient who has undergone SCS for axial or multi-dermatomal pain may develop a distinct peripheral nerve pain component that is not adequately covered by the existing SCS system, for which a separate PNS lead targeting the peripheral nerve is appropriate. In future care projections involving patients with both SCS and PNS systems, each device system must be projected separately with its own replacement schedule and programming cost structure.
- › Modality selection as a standard of care issue — When a physician implants SCS for a pain presentation that was most appropriately addressed at the peripheral nerve level, or conversely implants PNS for a multi-dermatomal pain pattern requiring SCS-level coverage, modality selection itself becomes a standard of care question. Expert review of neuromodulation cases must address whether the modality chosen was appropriate for the documented pain distribution and clinical presentation.
The Trial Stimulation Process
A PNS trial is the mandatory pre-implant assessment that evaluates the patient's response to peripheral nerve stimulation before permanent hardware is implanted. The trial involves percutaneous placement of a temporary lead adjacent to the target nerve — typically using ultrasound or fluoroscopic guidance to confirm proximity to the nerve — connected to an external pulse generator worn by the patient during the trial period. Trial duration for contemporary PNS devices typically ranges from three to seven days, though some protocols extend the trial period to more thoroughly assess the patient's response across activities of daily living.
The clinical endpoints for trial success must be defined in advance and documented in the pre-trial evaluation record. The standard threshold for a successful PNS trial is a minimum of 50% reduction in baseline pain intensity, as measured by a validated patient-reported outcome instrument (most commonly the Numeric Rating Scale or Visual Analog Scale) administered immediately before the trial lead is placed and at the conclusion of the trial period. Additional outcome metrics that strengthen the trial documentation include functional assessment using validated tools, documentation of analgesic medication use during the trial compared with baseline, and the patient's subjective assessment of whether the stimulation effect was sufficient to justify proceeding to permanent implantation.
- › Prognostic nerve block — A diagnostic nerve block targeting the proposed peripheral nerve target — performed before the PNS trial — provides preliminary evidence that the proposed nerve is the relevant pain generator. A positive block response (clinically meaningful temporary pain reduction correlated with the block distribution) supports the clinical rationale for targeting that nerve with PNS. Some institutions treat a positive prognostic nerve block as a required precondition to PNS trial; others use the trial itself as the definitive predictive assessment. The presence or absence of a documented prognostic block is a medical necessity consideration in cases where the nerve target selection is contested.
- › What adequate trial documentation requires — Adequate trial documentation in the clinical record consists of: the target nerve identified and the clinical rationale for that target; baseline pain scores recorded immediately before lead placement; the stimulation parameters programmed during the trial period; the patient's pain scores recorded at the end of the trial period; the physician's clinical assessment of the trial outcome including comparison of baseline and end-of-trial scores; and the documented decision to proceed to or defer permanent implantation based on the trial results. The absence of contemporaneous baseline scores — even if the physician characterizes the trial as successful in a narrative note — is an evidentiary gap that may not be bridged by retrospective recollection.
- › Failed trial — A documented trial that failed to meet the pre-specified success threshold should preclude permanent implantation without additional clinical justification. Proceeding to permanent implantation following a documented trial failure — or following a trial that was abandoned before the full trial period without clinical justification — is a recognized standard of care deviation. A record that documents an abbreviated trial without clinical explanation for early termination may not provide adequate support for a medical necessity determination.
The Permanent Implant Procedure
Permanent PNS implantation involves two principal surgical steps: placement of the permanent lead adjacent to the target nerve and creation of an implantable pulse generator pocket with connection of the lead to the IPG. The specific approach differs from SCS implantation in that the target is a peripheral nerve outside the spinal canal, and the lead placement must be performed at the anatomical location of the nerve rather than through the epidural space.
Percutaneous PNS lead placement — where the device platform and nerve anatomy allow — uses a needle-based approach under ultrasound and/or fluoroscopic guidance to advance the lead to the target nerve without open surgery. Open surgical placement is required when the target nerve is not accessible percutaneously, when precise surgical visualization is necessary to ensure adequate lead-nerve proximity, or when the lead is being placed in conjunction with other surgical procedures. The choice of placement approach affects the invasiveness and risk profile of the procedure and is a clinical judgment made by the implanting physician based on the specific device and anatomy.
The implantable pulse generator is typically placed in a subcutaneous pocket at a location accessible for future revision and battery replacement — commonly in the flank, buttock, or extremity depending on the location of the target nerve. Lead tunneling from the nerve site to the IPG pocket introduces a length of lead subcutaneous tunnel that is a potential site for infection and a mechanical constraint on lead movement.
Post-implant device programming — performed by the implanting or managing pain management physician — is required to optimize stimulation parameters for the individual patient. Programming visits in the immediate post-implant period and at subsequent intervals are a recurring clinical cost component of the PNS management plan and must be included in future care projections. Device programming complexity varies by device platform: some devices use proprietary programming software that requires a trained representative at programming visits, adding a cost component beyond the physician fee.
Medical Necessity Analysis
Medical necessity for PNS is evaluated against published clinical guidelines and the individual clinical record. A supported PNS implantation requires documentation of each threshold element of the selection criteria across the pre-implant record. Medical necessity review is performed from both directions: plaintiff review assesses whether the treating physician's record adequately documents the clinical basis for implantation; defense review evaluates whether each threshold element is present and whether the documented clinical course supports the decision to proceed to implantation at the time it was made. For the underlying examination methodology — range-of-motion assessment, sensory and motor testing, functional capacity evaluation, and validated outcome instruments — that a pain management physician uses to establish the clinical foundation for a PNS necessity opinion, see the article on how pain management experts objectively evaluate pain.
The six threshold elements of a medically supported PNS implantation are:
- › Diagnosis within a recognized indication — The patient's diagnosis must include a peripheral nerve-specific pain condition within the recognized PNS indication spectrum: peripheral nerve injury, neuroma, phantom limb pain, or CRPS Type II. A diagnosis of axial low back pain without a peripheral nerve-specific component does not support PNS as the primary treatment modality.
- › Documented conservative care failure — An adequate trial of pharmacological management with agents appropriate for neuropathic pain — including anticonvulsants such as gabapentin or pregabalin, SNRIs such as duloxetine, and tricyclic antidepressants — with documented clinical responses must precede implantation. Physical therapy and conventional interventional procedures — diagnostic and therapeutic nerve blocks — must also be documented with their outcomes. Implantation within weeks of the initial consultation, without a documented period of conservative management, is a recognized medical necessity concern.
- › Peripheral nerve confirmation — Electrodiagnostic evidence — nerve conduction velocity and electromyography — or clinical examination consistent with the proposed peripheral nerve injury should document that the proposed nerve is the relevant pain generator. The diagnostic nerve block result, when performed, provides additional functional confirmation.
- › Psychological evaluation — Pre-implant psychological screening by a licensed mental health provider is a standard of care requirement for PNS candidacy. The evaluation assesses untreated psychiatric comorbidities, active substance use disorder, cognitive capacity to manage the device, and psychosocial factors that may adversely affect PNS outcomes. Implantation without psychological clearance is a documented medical necessity gap.
- › Successful documented trial — The PNS trial must demonstrate a clinically meaningful response using pre-specified endpoints, with contemporaneous pain scores recorded at baseline and at trial conclusion, meeting the 50% improvement threshold. The trial result must be documented in the clinical record in a form that an independent reviewer can evaluate without relying solely on the treating physician's narrative characterization.
- › Medical clearance and contraindication review — Active systemic infection, coagulopathy, inability to comply with device programming or recharging (for rechargeable devices), and allergy to implant materials are contraindications requiring assessment. Patients on anticoagulation require planned anticoagulation management consistent with peripheral nerve procedure guidelines.
In personal injury future care analysis, medical necessity operates at a probabilistic level: the question is not whether the patient already meets the implantation threshold, but whether the documented clinical course makes PNS implantation a reasonably certain future need given the trajectory of the underlying condition. This requires prospective clinical judgment grounded in the documented record and supported by literature on the expected course of the underlying condition.
Standard of Care in PNS Management
The standard of care for peripheral nerve stimulation reflects the practice of a reasonably competent board-certified pain management physician with neuromodulation training, operating within published society guidelines and the clinical evidence base for PNS. Standard of care analysis in PNS litigation spans the full lifecycle of the device from patient selection through long-term management.
- › Appropriate candidate selection — The standard of care requires that the full pre-implant evaluation sequence — diagnosis confirmation, conservative care trial, psychological screening, diagnostic nerve block where indicated, and a successful documented stimulation trial — be completed before permanent implantation. Bypassing any element of this sequence, or proceeding to implantation on an accelerated timeline that cannot be clinically justified, is a recognized departure.
- › Appropriate modality selection — Selecting PNS for a pain presentation that lacks a discrete peripheral nerve substrate — or that would more appropriately be addressed by SCS — and selecting SCS for a presentation optimally addressed at the peripheral nerve level are both modality selection departures. Expert review must evaluate whether the documented pain distribution and clinical findings supported PNS as the most appropriate neuromodulation strategy.
- › Nerve target accuracy — The standard of care requires use of appropriate guidance — ultrasound and/or fluoroscopy — for percutaneous lead placement adjacent to the target nerve, and surgical exposure where percutaneous placement is not technically feasible for the target nerve anatomy. Inadequate stimulation coverage following implantation that is attributable to incorrect lead positioning relative to the target nerve is a technical standard of care concern.
- › Post-implant monitoring and complication recognition — After implantation, the standard of care includes periodic clinical follow-up, device interrogation and programming optimization, and prompt investigation of symptoms suggesting hardware complications — including unexplained loss of coverage, new pain at the lead site, or signs of infection. Failure to investigate symptoms suggesting lead migration or infection at an appropriate clinical stage is a recognized post-implant management departure.
- › Infection prevention — Perioperative prophylactic antibiotics, aseptic technique during trial lead placement and permanent implantation, and appropriate wound care instructions and follow-up are infection prevention standards applicable to PNS implantation. Failure to administer perioperative antibiotics or to use sterile technique during lead placement are documented departures in infection-related PNS malpractice claims.
Future Medical Care Projections
When PNS is proposed as future care in a personal injury damages analysis, the projection must address each cost component individually and ground each component in the documented clinical record, the implanted or proposed device specifications, and current market pricing in the patient's geographic area. Generic PNS future care projections that do not identify the device system, do not specify the battery replacement interval, or use non-market pricing are vulnerable to defense challenge.
A defensible future medical care projection for a PNS patient includes:
- › Trial stimulation cost — Pre-trial evaluation, temporary lead placement procedure (facility and physician fees), external generator rental if applicable, and trial period follow-up visits before the permanent implantation decision
- › Permanent implantation — Device hardware cost (specific to the selected device system), implanting physician fee, facility fee, anesthesia, and immediate post-operative care; varies by device system and geographic market
- › Battery replacement surgeries — Projected at device-specific intervals based on published longevity data at the documented stimulation parameters, with each replacement involving device, surgeon, facility, and anesthesia costs
- › Programming and follow-up visits — Post-implant programming sessions, periodic parameter optimization as the patient's condition evolves, and annual clinical assessments at the managing pain management practice
- › Lead revision allowance — A complication rate assumption grounded in published PNS literature for the probability of lead revision surgery over the projection period, not a zero-complication assumption and not an inflated rate unsupported by the literature
- › Ongoing pharmacological management — Continued management of the underlying neuropathic pain condition with pharmacological agents, even when PNS provides partial relief, is a recurring annual cost that should be itemized separately from device-related costs
Defense review of PNS future care opinions focuses on: whether the projected device system is identified and its specifications support the assumed cost and replacement interval; whether the replacement interval is based on device-specific data or a generic assumption; whether the geographic market pricing is supported; and whether any alternative management strategies were inappropriately excluded from the projection.
Battery Replacement and Device Longevity
Non-rechargeable PNS pulse generators contain finite-life batteries that must be surgically replaced when the device reaches end of battery life. Battery longevity is not a fixed number — it varies by device model, the stimulation amplitude and frequency programmed for the individual patient, and the duty cycle (the percentage of time stimulation is actually delivered). Devices programmed at higher output settings for patients with more severe neuropathic pain consume battery capacity at a faster rate and will reach end of battery life sooner than the same device programmed at lower settings for a milder presentation.
Each PNS device manufacturer publishes battery longevity data for their devices, typically provided as a range keyed to stimulation parameter combinations (amplitude, frequency, pulse width, and electrode configuration). The treating or prescribing physician's documentation of the actual programmed stimulation parameters is the clinical basis for estimating the specific replacement interval for a given patient. In the absence of programming records, the defense challenge is that the plaintiff's projections have used a conservative (short) battery life estimate that inflates the number of replacement surgeries over the projection period and overstates total replacement costs.
Rechargeable PNS devices avoid the periodic battery replacement surgery by using a rechargeable battery that is replenished via an external charging device. Rechargeable devices carry higher upfront costs but eliminate or extend the interval between replacement surgeries. The tradeoff is patient compliance: the patient must perform regular charging sessions (typically daily or every few days) to maintain adequate battery charge for continued device operation. Patient compliance with charging requirements is a clinical factor in device selection, and a patient who is unlikely to comply reliably with a charging protocol may not be an appropriate candidate for a rechargeable device.
In future care analysis, the choice between non-rechargeable and rechargeable device projections has significant cost implications over the patient's life expectancy. A future care projection that assumes a non-rechargeable device for a patient who is actually managed with a rechargeable device — or that uses a battery replacement interval shorter than what the device specifications and actual programming parameters support — overstates the long-term cost. Expert review of battery replacement projections requires knowledge of the specific device and the documented stimulation parameters.
Lead Migration
Lead migration — displacement of the PNS lead away from its intended position adjacent to the target nerve — is the most common hardware-related complication of peripheral nerve stimulation and a frequent source of both standard of care disputes and future care revision projections. Migration occurs when the lead shifts within the subcutaneous tissue due to patient movement, inadequate lead anchoring at the time of implantation, or gradual tissue displacement over time.
The clinical presentation of lead migration is a change in stimulation coverage: the patient reports that the paresthesia or sub-threshold stimulation that previously covered the pain distribution has shifted, diminished, or disappeared. Loss of stimulation coverage may occur acutely — from dislodgment of a recently placed lead — or gradually over weeks to months as the lead progressively moves from its initial position. The treating physician may attempt to compensate for mild migration through programming adjustments to shift the active electrode configuration, but significant migration that takes the lead beyond the range of programming compensation requires surgical revision.
- › Risk factors for migration — Lead migration risk is increased by inadequate anchoring of the lead at the time of implantation, high-mobility anatomical regions (leads near joints or over mobile soft tissue planes migrate more than leads in stable anatomical compartments), patient body habitus and activity level, and the specific mechanical design of the lead anchor system used by the device platform.
- › Standard of care implications — In malpractice matters where lead migration is alleged as a complication, expert review addresses: whether the lead was anchored using an appropriate anchoring technique at the time of implantation; whether the lead was placed in a region of high mobility without appropriate strain relief; whether the clinical signs of migration were recognized and investigated at an appropriate clinical stage; and whether revision surgery was offered in a timely fashion once migration was confirmed. Migration is a recognized risk of PNS rather than an inherently negligent outcome, but inadequate anchoring technique or failure to investigate symptoms of coverage loss may represent standard of care departures.
- › Future care implications — Published PNS literature documents lead revision rates that must be incorporated into future care projections. A future care projection that assumes zero lead revisions over the patient's lifetime is clinically unrealistic and subject to challenge; conversely, a projection that assumes an inflated revision rate above what the literature supports for the specific device type overstates future care costs. The appropriate revision rate assumption requires reference to published data for the specific device class used.
Revision Procedures
PNS revision surgery is required when lead migration, hardware failure, inadequate stimulation coverage, or device-related complications cannot be managed through programming adjustments alone. Revision procedures range in scope from minor lead repositioning — a relatively straightforward procedure to relocate a migrated lead under guidance — to complete hardware exchange involving removal of the existing lead system and IPG with replacement of new hardware.
The scope of the revision determines its cost. A lead repositioning procedure involves physician and facility fees, guidance fees (fluoroscopy or ultrasound), and anesthesia, but typically does not require a new lead or IPG if the existing hardware is intact. A complete hardware exchange — required when the existing lead is fractured, the IPG has malfunctioned, or the anatomy has changed such that the original implant position is no longer appropriate — involves the cost of new hardware in addition to the procedural fees.
- › Revision for inadequate coverage — When the initial permanent implant produces inadequate pain coverage despite appropriate programming — whether from lead-nerve distance, incorrect initial positioning, or individual anatomical variation — a revision to reposition the lead may be required. The distinction between inadequate coverage from suboptimal initial placement (a potentially preventable outcome) and inadequate coverage from individual anatomical variation (an inherent limitation) is a standard of care issue in malpractice cases alleging that the initial implant produced insufficient relief.
- › Revision for hardware failure — Lead fracture, connector failure, and IPG malfunction may require hardware exchange. Hardware failure resulting in loss of stimulation — particularly if the device is the patient's primary pain management strategy — represents a clinically meaningful harm that may require urgent revision. The manufacturer's known failure rate for the specific device is relevant to standard of care analysis when the failure mode was a known device issue.
- › Cost in future care — Each anticipated revision surgery adds a procedural cost component to the future care projection. The number of revisions projected over the patient's life expectancy must be grounded in published revision rates for the specific device type and placement location, not a generic or inflated assumption. Defense review of revision rate assumptions addresses whether the assumed revision rate is consistent with published literature for the device and anatomy involved.
Explantation
PNS explantation — complete surgical removal of the lead and IPG — may be required for infection, device malfunction that cannot be managed by revision, patient request, loss of clinical efficacy over time, or change in the patient's clinical condition that makes ongoing PNS management inappropriate. Explantation is also required when a patient undergoes MRI that is incompatible with the implanted device, in jurisdictions or clinical settings where the device manufacturer's MRI compatibility specifications are not met.
Explantation for infection is the most clinically urgent indication. Infection that involves the IPG pocket, the lead track, or presents as systemic infection in the setting of implanted hardware generally requires prompt explantation — antibiotic therapy alone is typically insufficient to eradicate infection in the presence of a foreign body. The explantation procedure removes both the infected IPG and the lead, followed by a prolonged course of antibiotics and a recovery period before reimplantation can be considered. The total harm in an infection explantation case includes the initial infection, the explantation surgery, the loss of the device that was providing pain control, the antibiotic course, and — if the patient subsequently requires reimplantation — the cost of repeating the full trial-to-implantation sequence.
In future care analysis, explantation is not typically projected as a routine future event unless the clinical record or device literature supports a specific explantation risk for the patient's presentation. However, when the record documents a prior explantation — and particularly when the reason for prior explantation suggests elevated risk of recurrence (chronic infection history, poor wound healing, prior implant failure) — the possibility of future explantation and reimplantation is a clinically supported future care component. Expert review must distinguish between a speculative explantation projection and one supported by the individual patient's clinical history and device literature.
PNS Cost Analysis
The aggregate lifetime cost of PNS therapy is a major component of damages in personal injury cases involving young patients with serious peripheral neuropathic pain. A complete, well-documented cost analysis enumerates and prices each cost component separately, with each component grounded in device specifications, published literature, and verifiable market pricing for the patient's geographic location.
- › Pre-implant evaluation costs — Electrodiagnostic studies, psychological evaluation, diagnostic nerve blocks, pre-implant consultation visits, and pre-authorization processes before the trial and implantation are upfront costs that precede device placement
- › Trial stimulation costs — Temporary lead placement procedure (facility, physician, and guidance fees), external generator, and trial follow-up visits constitute the trial phase costs
- › Permanent implantation — Device hardware cost (non-rechargeable PNS systems vary considerably in price by manufacturer and model), physician fee, facility fee, anesthesia, and post-operative care; must be priced for the specific device system, not generically
- › Battery replacement over life expectancy — The number of replacements is calculated from (life expectancy − age at implant) ÷ device battery life at documented parameters; each replacement is priced at hardware + surgeon + facility + anesthesia costs for the replacement procedure
- › Ongoing programming and clinical follow-up — Post-implant programming visits (typically more frequent in the first year, then annually), medication management for the underlying pain condition, and periodic clinical assessments; annual recurring cost component
- › Lead revision allowance — A revision probability per device cycle applied to the replacement interval to project the expected number of lead revision procedures over the life expectancy; must be based on published literature for the specific device class
- › Pharmacological management — Ongoing neuropathic pain medications — even when PNS provides partial relief, adjunct pharmacological management is typically maintained — priced at current market rates for the prescribed agents
Defense cost analysis challenges commonly focus on three areas: (1) whether the assumed battery replacement interval is shorter than what the device specifications support at the patient's actual stimulation parameters; (2) whether the device hardware pricing reflects current market pricing rather than list pricing; and (3) whether the revision rate assumption is supported by the literature for the specific device and anatomy involved.
Causation Analysis
Causation analysis in PNS cases operates at two distinct levels that must each be established to support PNS damages attribution in personal injury litigation.
The first level is peripheral nerve causation: establishing that the underlying peripheral nerve injury, neuroma, or CRPS Type II that generates the PNS indication is causally attributable to the subject incident. This analysis requires: review of the mechanism of the subject incident and its anatomical plausibility as a cause of peripheral nerve injury at the claimed location; evaluation of the pre-injury clinical record for baseline peripheral nerve pathology; the temporal relationship between the incident and the onset of neuropathic symptoms; electrodiagnostic evidence of peripheral nerve injury consistent with the claimed mechanism; and clinical examination findings in the expected distribution of the claimed nerve injury.
The second level is treatment causation: establishing that, given the causally related peripheral nerve condition, PNS implantation is a medically appropriate and reasonably certain component of the future treatment course. Treatment causation requires that the clinical record document a trajectory of escalating treatment for the peripheral neuropathic pain that makes eventual PNS candidacy reasonably certain — conservative management, interventional procedures, and progressive refractory pain consistent with PNS indication criteria.
Pre-existing peripheral nerve pathology introduces a specific causation challenge. Patients with baseline peripheral neuropathy, prior peripheral nerve injuries, or pre-existing CRPS require causation analysis that specifically distinguishes the pre-existing condition from the incident-related pathology. Aggravation causation — the subject incident materially accelerated, exacerbated, or worsened a pre-existing peripheral nerve vulnerability — is a recognized theory that can support PNS damages attribution even where the patient's peripheral nervous system was not entirely intact before the incident.
In malpractice matters where an iatrogenic surgical complication caused the peripheral nerve injury underlying the PNS indication, causation analysis addresses the specific mechanism of the nerve injury, whether it was a recognized complication or a consequence of a technical departure, and whether the nerve injury and its downstream consequences — including eventual PNS candidacy — are within the causal chain of the alleged malpractice.
IME Considerations
Independent medical evaluation of a PNS patient — or a claimant for whom PNS is proposed as future care — requires a structured examination adapted to the specific clinical questions at issue. The scope and format of the examination are determined by whether PNS is already implanted or is proposed as future care, and by the specific questions retaining counsel needs addressed.
When PNS is already implanted, examination includes: neurological assessment of the extremity in the nerve's distribution, documenting sensory findings (allodynia, hyperalgesia, hypesthesia, or sensory loss), motor findings where relevant, and trophic changes; palpation and visual inspection of the IPG pocket site and lead entry site for signs of infection, erosion, or hardware palpability; and functional assessment of the patient's performance on examination relative to the claimed pain level and functional limitation. Examination findings inconsistent with the claimed level of disability or the expected clinical profile of the peripheral nerve injury are relevant to both damages and causation opinions.
When PNS is proposed as future care, the examination focuses on the current clinical status of the underlying peripheral neuropathic condition — documenting the distribution and character of symptoms, the neurological examination findings supporting peripheral nerve involvement, and the current treatment status. The examination findings must support the clinical proposition that the patient's condition is on a trajectory toward PNS candidacy, or must identify reasons why PNS candidacy is not supported on current examination.
Records-based review — without in-person examination — is appropriate for many PNS medical-legal engagements when the questions concern medical necessity, trial documentation adequacy, standard of care for device management, or future care cost analysis and the current clinical status does not need to be independently assessed. The appropriate engagement format is determined by the specific questions to be addressed, not by a default preference for either records review or examination.
Common Litigation Issues in PNS Cases
PNS matters in personal injury and medical malpractice litigation present a defined set of recurring clinical issues that require case-specific expert analysis.
- › Personal injury — PNS as proposed future care — A plaintiff with refractory peripheral neuropathic pain from a traumatic nerve injury whose treating pain management physician recommends PNS as the next treatment step. The plaintiff's life care plan projects PNS trial, implantation, battery replacement, and revision costs over the plaintiff's life expectancy. Defense review addresses whether the clinical course supports the PNS recommendation, whether the prior treatment pathway is adequately documented, and whether each projected cost component is individually supported and appropriately priced.
- › Malpractice — premature implantation — A patient undergoes permanent PNS implantation before completing an adequate conservative care trial, without psychological clearance, or after a trial that failed to meet the documented success threshold. The claim addresses whether the premature implantation represented a departure from the standard of care and whether the patient suffered harm — including the risks of the implantation surgery, subsequent complications, and the financial burden of the device — as a result of that departure.
- › Malpractice — lead migration with loss of coverage — A patient's PNS lead migrates from its initial position, resulting in loss of stimulation coverage and return of neuropathic pain. The claim addresses whether the lead was adequately anchored at the time of implantation, whether clinical symptoms of migration were recognized and investigated promptly, and whether revision was offered in a clinically appropriate timeframe.
- › Malpractice — infection requiring explantation — A PNS infection develops — at the lead entry site, the pocket, or along the lead track — requiring explantation, antibiotics, and a period without device therapy. The claim addresses whether infection prevention measures were appropriate, whether the infection was recognized and managed promptly once identified, and whether management decisions delayed or complicated resolution. Explantation and reimplantation costs, and the harm of the period without device therapy, are included in damages.
- › Damages dispute — device cost and replacement schedule — A defense challenge to the plaintiff's life care plan that argues the projected battery replacement interval is too short based on the specific device's published specifications at the patient's programmed parameters, or that the projected cost per replacement procedure uses list pricing rather than market pricing. Expert review resolves the dispute by applying device-specific published longevity data to the documented stimulation parameters and current market pricing in the patient's geographic area.
Attorney FAQ: Retaining a PNS Expert
-
What records are needed for a PNS expert review?
A complete PNS records review requires: all treating pain management records from the beginning of the pain management relationship; pre-implant evaluation records including electrodiagnostic studies and psychological evaluation; diagnostic nerve block procedure records with documented responses; PNS trial procedure records including pre-trial and post-trial pain scores; permanent implant operative report with documented lead placement and device information; post-implant device programming records; any imaging studies including X-rays documenting lead position; records of any complications, revisions, or explantations; and prior treating records for the underlying injury and any pre-existing conditions. For damages-focused engagements, billing and authorization records are also useful.
-
Can PNS expert review be provided on short notice?
Availability depends on current case volume. Contact Expert Medical Services LLC with a brief case summary and the timeline required. Expedited review may be available for cases with imminent trial or deposition dates; advance scheduling is preferred for comprehensive records review engagements.
-
What specific questions can a PNS expert address?
Expert opinions can be structured to address: medical necessity of the PNS trial and permanent implantation; standard of care for patient selection, trial conduct, and device management; causation of the underlying peripheral nerve condition; adequacy of trial documentation; lead migration or infection standard of care; future medical care projections including device, replacement, revision, and management costs; and critique or defense of opposing expert opinions on PNS-related issues. Engagements may address all of these questions or a defined subset based on the issues in the case.
-
Can Dr. Dardashti review PNS cases in California, Texas, and Nevada?
Yes. Dr. Dardashti accepts PNS engagements in California, Texas, Nevada, and nationally. He is California-based and available for deposition and trial testimony in state and federal courts nationwide.
Related Services & Expertise
Peripheral Nerve Injury
The primary underlying injury condition giving rise to PNS candidacy in personal injury litigation.
CRPS / RSD
CRPS Type II — with a confirmed peripheral nerve substrate — is a recognized PNS indication distinct from CRPS Type I.
Spinal Cord Stimulation
A related implantable neuromodulation modality with broader dermatomal coverage — modality selection is a standard of care issue.
Amputation & Phantom Limb Pain
Post-amputation neuroma pain and phantom limb pain are recognized PNS indications in high-value personal injury cases.
Causation Analysis
Linking the peripheral nerve injury or CRPS Type II underlying PNS candidacy to the subject incident.
Future Medical Care Review
PNS trial, implantation, battery replacement, and revision cost projections for personal injury damages.
Intrathecal Pump Therapy
An alternative implantable modality for refractory chronic pain when neuromodulation at the peripheral level is inadequate.
Arizona Pain Management Expert Witness
Peripheral nerve stimulation expert review for Arizona personal injury litigation.
Florida Pain Management Expert Witness
Peripheral nerve stimulation expert review for Florida personal injury and medical malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for peripheral nerve stimulation — candidacy criteria, trial documentation, and implant justification.
Standard of Care Analysis
Standard of care analysis for PNS patient selection, trial protocol, and permanent implant decision-making.
FAQ
Peripheral Nerve Stimulation — Common Attorney Questions
- Peripheral nerve stimulation (PNS) is an implantable neuromodulation procedure in which electrical leads are placed adjacent to a specific peripheral nerve outside the spinal canal. Programmable electrical stimulation delivered through those leads modulates pain signaling at the peripheral nerve level — upstream from the spinal cord — producing analgesia in the targeted nerve's distribution. PNS arises in litigation as proposed future care in personal injury damages analysis, as a disputed medical necessity item in insurance matters where the prior conservative care trial is contested, and as the subject of standard of care review involving device complications, lead migration, infection, or allegations of premature implantation without adequate prior management.
- PNS is indicated for refractory neuropathic pain localized to the territory of a specific peripheral nerve that has failed conservative pharmacological and interventional management. Recognized indications in the litigation context include: traumatic peripheral nerve injury from motor vehicle accidents, workplace incidents, or surgical complications; neuroma pain from post-amputation or post-surgical nerve division; phantom limb pain refractory to conventional management; and Complex Regional Pain Syndrome Type II — which, unlike CRPS Type I, has a confirmed peripheral nerve substrate that provides an anatomically defined PNS target. The distinction between CRPS Type I and Type II is clinically material to PNS candidacy because PNS is most directly justified when the peripheral nerve substrate of the pain is defined.
- Spinal cord stimulation targets the dorsal columns of the spinal cord and produces broad segmental paresthesia coverage across a dermatomal territory. Peripheral nerve stimulation targets a discrete named peripheral nerve outside the spinal canal, producing stimulation confined to the distribution of that nerve. PNS is most appropriate when pain is localized to the territory of a specific, identifiable nerve — such as the sural nerve, saphenous nerve, or radial sensory nerve — rather than a broad multi-dermatomal distribution. SCS is generally preferred for axial or multi-dermatomal patterns where a central target is more efficient; PNS is preferred when the pain generator is identifiable at the peripheral nerve level. Selecting the wrong modality for the clinical presentation — SCS when PNS is indicated, or PNS when the pain does not have a discrete peripheral nerve substrate — is a standard of care issue. The two modalities are complementary rather than interchangeable, and a patient who has failed SCS may remain a candidate for PNS when the pain has a defined peripheral nerve component.
- Peripheral nerve stimulation delivers sub-threshold electrical current to sensory fibers in a peripheral nerve, modulating nociceptive signal transmission through several convergent mechanisms. Gate control theory — first described by Melzack and Wall — explains the analgesic effect of activating large-diameter Aβ touch fibers, which inhibit transmission of pain signals from small-diameter C and Aδ nociceptors at the same segmental level. More recent evidence supports additional mechanisms: antidromic and orthodromic effects on peripheral nociceptor sensitization, reduction in inflammatory neuropeptide release from peripheral nerve terminals, and central modulation of descending inhibitory pathways that are activated by sustained peripheral nerve stimulation. The net clinical effect is reduction in ongoing spontaneous neuropathic pain and diminished allodynia and hyperalgesia in the stimulated nerve's distribution. These mechanistic considerations are relevant in malpractice matters when questions arise about why a PNS device produced insufficient coverage — whether the mechanism was inadequate for the clinical presentation or whether device placement or programming was suboptimal.
- Medical necessity for PNS requires documentation of six threshold elements in the clinical record: (1) a diagnosis with a peripheral nerve substrate within a recognized PNS indication category; (2) electrodiagnostic or clinical evidence confirming peripheral nerve involvement as the pain generator; (3) an adequate documented trial of pharmacological management using agents appropriate for neuropathic pain — including anticonvulsants, SNRIs, and tricyclic antidepressants — with documented responses; (4) documentation of appropriate interventional pain procedures such as diagnostic and therapeutic nerve blocks; (5) psychological evaluation clearance for implantable device candidacy; and (6) a successful, documented PNS trial meeting pre-specified efficacy thresholds — typically at least 50% reduction in baseline pain — before permanent implantation. The absence of any of these elements in the clinical record is a recognized medical necessity gap subject to challenge in litigation.
- The PNS trial is a mandatory pre-implant assessment in which a temporary lead is placed percutaneously adjacent to the target nerve and connected to an external pulse generator for a defined period — typically three to seven days for contemporary percutaneous devices, though some protocols involve longer externalized lead trials. A successful trial is defined by pre-specified clinical endpoints, most commonly a minimum of 50% reduction in pain intensity as measured by a validated patient-reported scale (VAS or NRS) from pre-trial baseline. Additional success criteria may include functional improvement and reduction in analgesic medication requirements. In litigation, the trial documentation is the single most important record for medical necessity review: a permanent implant that proceeded without documented baseline and post-trial pain scores, or where the documented trial failed to meet the 50% threshold, cannot be supported on medical necessity grounds regardless of the treating physician's clinical narrative. Defense review routinely identifies cases where the trial proceeded but the documentation is insufficient to establish success.
- Recognized PNS complications requiring standard of care analysis include: lead migration — displacement of the lead away from the target nerve resulting in loss of stimulation coverage, which is the most common hardware complication and may require revision surgery; infection at the lead entry site, pocket site, or along the lead track, ranging from superficial wound infection to deep tissue infection requiring lead explantation; seroma or hematoma formation at the pocket site; inadequate stimulation coverage from incorrect initial lead positioning; nerve injury from lead placement at or near the target nerve; and hardware failure requiring device revision. In each complication type, expert review addresses whether the complication was a recognized and accepted risk managed appropriately once identified, or whether the occurrence or management represented a deviation from the standard of care — in patient selection, technical placement, perioperative management, or post-operative monitoring.
- Non-rechargeable PNS devices require periodic surgical battery replacement when the implantable pulse generator reaches end of battery life. Battery longevity varies by device manufacturer, model, and the stimulation parameters programmed — devices running at higher output and frequency consume more battery capacity per unit time. Published device-specific battery longevity ranges provide the basis for the replacement interval in future care projections. Each battery replacement involves a surgical procedure to explant the depleted IPG and implant a replacement device, with associated device cost, surgeon fee, facility fee, and anesthesia. Over the life expectancy of a young patient, battery replacements may represent the largest cumulative surgical cost component of a PNS future care projection. Defense review addresses whether the replacement interval is based on device-specific published data at documented stimulation parameters, rather than a generic or pessimistic assumption that inflates the replacement frequency and total projected cost.
- Causation analysis in PNS future care cases operates at two levels. The first is peripheral nerve causation: whether the underlying peripheral nerve injury, neuroma, or CRPS Type II that gives rise to PNS candidacy is causally linked — as a direct or aggravated result — to the subject incident. This analysis requires review of the mechanism of injury, electrodiagnostic evidence of peripheral nerve injury, the anatomical plausibility of the proposed causal mechanism, and the temporal relationship between the incident and the onset of neuropathic symptoms. The second is treatment causation: whether, given the documented clinical course of that causally related condition, PNS implantation is a medically appropriate and reasonably certain component of future treatment. PNS as future care cannot be attributed to a defendant if the underlying condition generating the PNS indication is not itself causally linked to the incident. Pre-existing peripheral nerve pathology — including prior nerve injuries, baseline neuropathy, or pre-existing CRPS — requires specific causation analysis distinguishing pre-existing from incident-related pathology.
- Yes. Dr. Dardashti accepts PNS engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice review for both sides. Engagements may address medical necessity, standard of care for device selection and management, trial stimulation adequacy, lead migration and other complication review, causation of the underlying condition, and future medical care projections — or a defined subset based on the specific questions retaining counsel needs addressed. Contact Expert Medical Services LLC with a brief case summary confirming the available records, the questions to be addressed, and the jurisdiction, to discuss scope and availability.
Retain Dr. Dardashti for a Peripheral Nerve Stimulation Matter
Dr. Dardashti accepts peripheral nerve stimulation engagements for plaintiff and defense. Contact Expert Medical Services LLC to discuss case scope and availability.