Nationwide Pain & Injury Medical Expert Witness
Post-Laminectomy Syndrome Expert Witness
Expert evaluation of persistent spinal pain following surgery — causation, treatment necessity, standard of care, spinal cord stimulation, and future medical care in complex personal injury and malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Condition
- Post-Laminectomy Syndrome (PLSS)
- Also Known As
- Persistent Post-Surgical Spinal Pain
- Specialty
- Pain Management & Anesthesiology
- Evaluation Areas
- Causation, Standard of Care, Treatment Necessity, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Post-Laminectomy Syndrome in Medical-Legal Review
Post-laminectomy syndrome is persistent or recurrent spinal pain that continues following spinal surgery — including laminectomy, discectomy, spinal fusion, or combined procedures — in the absence of a recognized intraoperative complication. It is one of the most clinically complex and medico-legally significant diagnoses in personal injury and malpractice litigation involving spinal injuries, and it is the most common indication for spinal cord stimulation implantation in the United States.
The name post-laminectomy syndrome reflects historical terminology from an era when laminectomy was the predominant spinal surgical approach. The condition encompasses persistent post-surgical pain following any spinal procedure — discectomy, foraminotomy, fusion, or multi-level decompression. In the contemporary medical-legal setting, the term is used broadly to describe post-surgical spinal pain syndromes regardless of the specific procedure performed.
In litigation, post-laminectomy syndrome arises most commonly in two contexts. In personal injury matters, a traumatic event leads to spinal surgery and the patient develops persistent post-surgical pain — raising questions about causation, the clinical basis for surgery, the adequacy of post-operative pain management, and future care needs including the potential need for spinal cord stimulation. In medical malpractice matters, questions arise about the post-surgical standard of care — whether persistent pain was appropriately recognized, evaluated, and managed, and whether a timely referral to pain management was made. Expert review is case-specific and is grounded in the available medical records and the scope defined by retaining counsel.
What Is Post-Laminectomy Syndrome?
Post-laminectomy syndrome is a clinical diagnosis assigned when a patient who undergoes spinal surgery for a structural indication — disc herniation, spinal stenosis, spondylolisthesis, or segmental instability — continues to experience significant spinal pain after surgery, or when pain that initially improved following surgery later returns. The diagnosis does not imply surgical error. It reflects the documented clinical reality that spinal surgery addresses identifiable structural pathology but does not uniformly resolve the chronic pain state, and that a subset of patients develop new or secondary pain mechanisms following the surgical intervention itself.
Post-surgical spinal pain can take several forms. Some patients experience radicular pain — pain radiating into the lower extremity in a dermatomal pattern consistent with nerve root involvement — that persists despite technically successful decompression. Others experience primarily axial pain — back or neck pain at the surgical level — without significant radicular symptoms. Still others develop a mixed pattern, with both axial and radicular components that may arise from different post-surgical pain generators and require different treatment approaches.
The distinction between radicular and axial post-surgical pain matters clinically and medico-legally because the underlying mechanisms, the appropriate treatments, and the future care projections differ materially between the two presentations. Radicular post-surgical pain may respond to epidural injections, SCS with radicular paresthesia coverage, or targeted nerve procedures. Axial mechanical post-surgical pain — from facet joint pain, pseudarthrosis, or hardware-related pain — may respond to medial branch blocks, radiofrequency ablation, or surgical revision. A treating pain management physician who does not distinguish between these presentations and document that distinction may not be providing — or documenting — care consistent with the standard. For the full clinical evaluation methodology — examination components, imaging correlation, validated functional instruments, and symptom validity assessment — that governs the standard-of-care expectation for post-surgical pain evaluation, see the article on how pain management experts objectively evaluate pain.
Neuropathic pain is a third clinical dimension. Even when structural causes of post-surgical pain have been identified and addressed, central sensitization — a state of amplified and persistent pain processing driven by neuroplastic changes in the spinal cord and brain — can perpetuate pain independent of ongoing structural pathology. The presence of central sensitization affects treatment planning, the prognosis for improvement with additional surgery or interventional procedures, and the clinical basis for advanced neuromodulation. Identifying central sensitization as a component of the post-surgical pain syndrome is a distinct and clinically important element of expert review.
Causes of Persistent Pain After Spinal Surgery
Multiple distinct mechanisms can produce or perpetuate post-surgical spinal pain. Identifying the operative mechanism — or the combination of mechanisms — present in a given patient is a foundational element of both clinical management and expert record review. The following are the most clinically and medico-legally significant:
- › Epidural fibrosis — The formation of scar tissue within the epidural space around nerve roots is a normal biological response to spinal surgery. In some patients, the scar tissue is extensive enough to mechanically tether or compress a nerve root, producing radicular pain that is clinically indistinguishable from recurrent disc herniation. Epidural fibrosis is one of the most commonly identified contributors to post-surgical radicular pain and is a recognized non-surgical indication for interventional pain management and, in refractory cases, spinal cord stimulation. It is visible on MRI as a mass of enhancing tissue surrounding the nerve root on gadolinium-enhanced imaging, though imaging findings do not always correlate with clinical severity. In the litigation context, the distinction between epidural fibrosis-related pain and recurrent disc herniation has implications for treatment appropriateness analysis, because additional surgery for epidural fibrosis generally carries a poor prognosis for pain relief.
- › Recurrent disc herniation — Reherniation at the same level that was previously operated on occurs in a clinically significant subset of patients following discectomy. Recurrent herniation produces a clinical picture similar to the original presentation — dermatomal radicular pain, positive straight-leg raise, and imaging findings consistent with nerve root compression — but in the post-surgical context the physical examination may be more difficult to interpret due to post-surgical scarring and altered anatomy. In personal injury matters where a second surgery is performed for recurrent herniation, the causal analysis must address whether the recurrent herniation represents a new structural failure from the same traumatic mechanism, a natural consequence of the prior discectomy, or an unrelated degenerative event.
- › Adjacent segment disease — Spinal fusion surgery eliminates motion at the fused segment and transfers increased mechanical load to the immediately adjacent unfused levels. Over time, this altered biomechanical environment can accelerate disc degeneration, facet arthrosis, and the development of stenosis at the adjacent levels — a pattern called adjacent segment disease. Adjacent segment disease typically manifests years to decades following fusion surgery and may require further surgical intervention. In litigation, it arises in future care analysis for patients who have undergone fusion surgery for traumatic spinal injury, and in malpractice matters where the indication for fusion — and the decision to fuse rather than use a motion-preserving approach — is questioned.
- › Failed fusion — pseudarthrosis — Pseudarthrosis occurs when the bone graft placed during fusion surgery does not achieve the intended solid bony union. The resulting lack of segmental stability produces continued mechanical pain at the fusion level, often with characteristic features of instability pain that is worsened by loading activities and relieved by rest. On imaging, pseudarthrosis may be visible as the absence of trabecular bridging across the fusion site, though CT scan with specific reformatting is more sensitive than MRI for pseudarthrosis detection. Clinically, the presence of pseudarthrosis may explain post-surgical mechanical pain that persists despite an otherwise adequate decompression, and it is a recognized indication for revision fusion surgery. In litigation, pseudarthrosis is relevant both as a potential basis for malpractice — if the fusion technique, graft selection, or post-operative activity instructions deviated from the standard — and as a future care element if revision surgery is anticipated.
- › Hardware-related pain — Spinal instrumentation — pedicle screws, connecting rods, interbody cages, and dynamic stabilization devices — can produce localized mechanical pain from hardware prominence, screw loosening, screw fracture, or hardware migration. Symptomatic hardware pain may require revision surgery for hardware removal or adjustment. The presence of hardware-related pain is relevant in litigation when the treating physician has not distinguished between hardware-related and central post-surgical pain, when hardware failure has occurred and the adequacy of the surgical technique is at issue, or when future hardware removal surgery is projected as a future care element.
Neuropathic Pain Following Spinal Surgery
Neuropathic pain is a clinically distinct component of post-laminectomy syndrome that arises from injury to, or pathological sensitization of, the neural structures involved in spinal pain signaling. It is characterized by burning, electric, or shooting quality pain; allodynia (pain from non-painful stimuli such as light touch or clothing contact); hyperalgesia (exaggerated pain responses to normally painful stimuli); and a pain distribution that may extend beyond the expected anatomical territory of the structural pathology identified on imaging.
Nerve root injury during spinal surgery — from surgical retraction, epidural hematoma, or direct trauma — can produce a post-surgical neuropathic pain state that persists long after the structural insult has resolved. This is distinct from CRPS Type II, which requires a confirmed peripheral nerve injury and a broader clinical syndrome, though post-surgical nerve root injury can in some cases precipitate a CRPS-like syndrome in the affected extremity. The distinction between post-surgical radiculopathy, post-surgical peripheral nerve injury, and CRPS Type II arising after spine surgery is a specific area of expert review in complex spinal malpractice and personal injury matters.
Central sensitization — a state of persistent central nervous system hyperexcitability driven by chronic pain signaling — is recognized as a significant contributor to post-laminectomy syndrome in patients with long-standing pre- and post-surgical pain. Central sensitization explains why pain persists and may intensify even when structural pathology has been surgically addressed, and why further surgery often does not provide relief in patients with established central sensitization. Its presence is relevant to both the prognosis and the treatment planning analysis in expert review — specifically, whether additional surgical or interventional approaches are likely to be effective, or whether the clinical trajectory supports escalation to advanced neuromodulation therapies.
Medical Necessity and Treatment Escalation
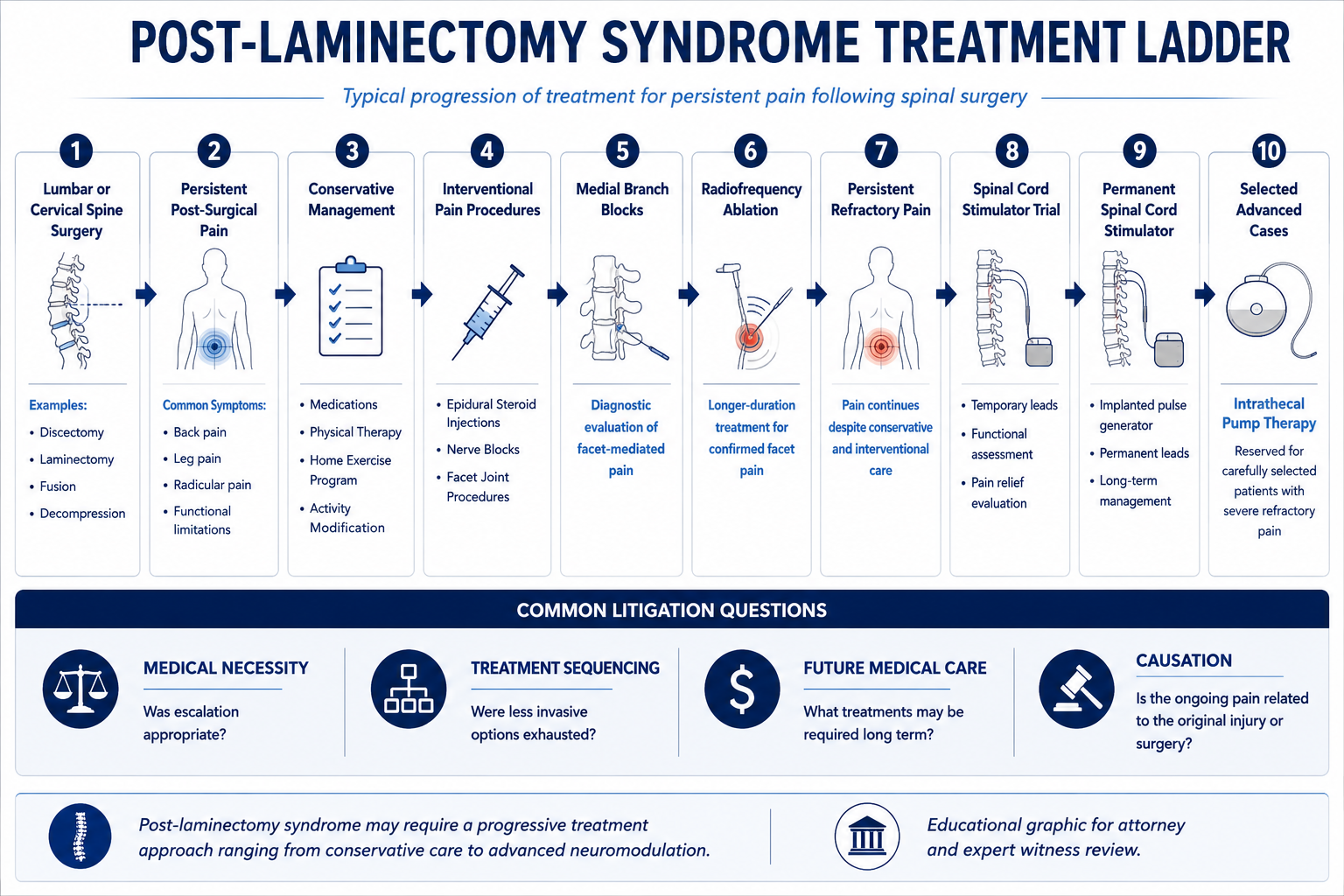
Post-laminectomy syndrome is treated through a graduated escalation of interventional and pharmacological approaches matched to the specific pain generators identified. Medical necessity review evaluates whether the treatments rendered or proposed are consistent with recognized clinical practice for the documented post-surgical pain pattern.
First-line pharmacological management for post-surgical neuropathic and mixed pain typically includes calcium channel modulators (gabapentin, pregabalin), tricyclic antidepressants, serotonin-norepinephrine reuptake inhibitors (duloxetine), and anti-inflammatory agents where appropriate. Opioid analgesics may be used for acute post-surgical pain and in selected cases for chronic management, but their long-term role in PLSS is limited by concerns about opioid-induced hyperalgesia, tolerance, and functional interference. The rationale for the medications prescribed, the documented clinical response to each agent, and the basis for any medication changes are reviewed in both necessity and standard of care analysis.
Interventional pain procedures in post-laminectomy syndrome are selected based on the dominant pain generator. Epidural steroid injections — transforaminal or interlaminar — are appropriate for radicular post-surgical pain with evidence of ongoing nerve root irritation or inflammation, and their medical necessity is evaluated against the specific clinical and imaging findings at the treated level. Medial branch blocks and radiofrequency ablation are appropriate for facet-mediated axial pain components that are distinct from the radicular pain pattern. The diagnostic pathway to RFA — two confirmatory blocks with adequate documented relief — applies equally in the post-surgical context.
When conservative and conventional interventional management fails to provide adequate relief, escalation to advanced neuromodulation is considered. The adequacy of the conservative care trial is a threshold element of the necessity analysis for advanced therapies. A treating physician who proceeds to spinal cord stimulation without documented failure of appropriate conservative management faces both standard of care and medical necessity challenges. Conversely, a patient with a well-documented conservative treatment course that has clearly failed — with contemporaneous records of each treatment's response — provides the strongest foundation for a medical necessity opinion supporting SCS or intrathecal drug delivery.
Spinal Cord Stimulation for Post-Laminectomy Syndrome
Spinal cord stimulation is the most evidence-supported advanced treatment for post-laminectomy syndrome and represents the primary clinical pathway for patients with PLSS who have failed conservative and conventional interventional management. Multiple randomized controlled trials and long-term observational studies have demonstrated superior pain relief and functional improvement with SCS compared to reoperation and continued conventional medical management in appropriately selected PLSS patients.
The indication for SCS in PLSS is best supported in patients with a dominant radicular pain component — persistent leg or arm pain in a dermatomal distribution consistent with nerve root involvement — where the radicular pain has not responded to epidural injections, pharmacological management, and physical therapy. SCS lead placement targets the dorsal columns at the thoracic or cervical level corresponding to the pain distribution, and the goal is to produce paresthesia coverage — or in newer waveform systems, sub-perception modulation — in the painful extremity distribution. Axial back pain as the primary PLSS presentation has a less robust evidence base for SCS than radicular-dominant PLSS, and medical necessity analysis must address whether the specific pain pattern is consistent with the published evidence for SCS efficacy.
Pre-implant evaluation requirements are identical to SCS for other indications: a documented history of failure of appropriate conservative care; psychological screening by a qualified mental health provider; and a successful trial stimulation period — typically seven to ten days — during which the patient evaluates pain relief in the ambulatory setting before permanent device implantation is authorized. A successful trial is generally defined as at least 50% reduction in pain intensity with contemporaneous documentation of pre-trial and post-trial pain scores. Absence of adequate trial documentation, or permanent implantation without a completed trial, are recognized medical necessity and standard of care issues.
In personal injury litigation where a traumatic event has led through spinal surgery to post-laminectomy syndrome requiring SCS, the aggregate future care costs are substantial. Trial stimulation, permanent implantation, battery replacement cycles at intervals determined by device type (rechargeable vs. non-rechargeable), revision procedures at rates consistent with published hardware complication literature, and ongoing programming visits each constitute distinct line items in a comprehensive future medical care projection. The total cost of SCS over a patient's life expectancy is a significant driver of damages in high-value spinal injury cases.
Standard of Care Considerations
The standard of care for post-laminectomy syndrome management reflects the practice of a reasonably competent pain management physician evaluating a patient with persistent post-surgical spinal pain. Expert review addresses whether the care provided met this standard — it does not address neurosurgical technique, surgical indication, or the spinal surgery standard of care, which require a spine surgeon expert.
- › Comprehensive initial evaluation — The initial pain management evaluation of a post-surgical patient should document the character, location, and radiation pattern of pain; distinguish between radicular and axial components; correlate the pain pattern with available post-surgical imaging; review the surgical operative report and post-operative records; assess functional status; and identify any psychological comorbidities relevant to treatment planning. An evaluation that proceeds directly to interventional procedures without this foundational characterization does not meet the standard for complex post-surgical pain assessment.
- › Pain generator identification — Appropriate management requires identifying the predominant pain generator — epidural fibrosis, recurrent pathology, facet-mediated pain, hardware pain, or central sensitization — before selecting treatment. Treating a patient with axial mechanical post-surgical pain with serial epidural steroid injections, or a patient with radicular pain from epidural fibrosis with RFA, reflects a mismatch between diagnosis and treatment that is relevant to both necessity and standard of care analysis.
- › Graduated treatment approach — Standard PLSS management follows a treatment escalation ladder from conservative and pharmacological management through interventional procedures and, where indicated, advanced neuromodulation. Premature escalation to high-cost or high-risk interventions without an adequate trial of less invasive treatment, or failure to escalate when conservative measures have demonstrably failed, are both standard of care considerations.
- › Opioid management documentation — Long-term opioid therapy for post-surgical spinal pain requires documented informed consent, a prescription monitoring program check, urine drug screening at clinically appropriate intervals, periodic reassessment of treatment goals and functional status, and a documented rationale for continuing opioid therapy when function is not improving. Opioid management that lacks these documentation elements is potentially below the standard of care regardless of whether the patient's pain is genuine.
- › Pre-SCS evaluation compliance — When SCS is recommended, the pre-implant evaluation sequence — documented conservative care failure, psychological screening, and a successful trial — is a standard of care requirement. Proceeding to permanent SCS implantation without any component of this sequence is a recognized deviation, and the adequacy of each component is subject to review in necessity and malpractice matters.
- › Referral obligations — A primary care physician or spine surgeon managing a post-surgical patient with persistent pain has an obligation to refer to pain management when the post-surgical pain is not responding to standard post-operative analgesic management within a clinically appropriate timeframe. Failure to recognize persistent post-surgical pain as a distinct clinical problem requiring pain management evaluation — and to refer accordingly — is a standard of care issue in malpractice matters where delayed treatment is alleged to have worsened outcomes.
Common Litigation Issues
Post-laminectomy syndrome cases present a defined set of litigation issues that arise across personal injury and medical malpractice contexts. Understanding these patterns informs the records to obtain and the specific questions that expert review should address.
- › Causation of the underlying spinal injury — Whether the subject accident produced or materially aggravated the spinal pathology that required surgery is the foundational causation question. Pre-existing degenerative spinal disease is common in adults and does not preclude accident-related causation; it requires a specific analysis of whether the subject event caused new structural injury, aggravated a symptomatic pre-existing condition, or accelerated an asymptomatic degenerative condition to become symptomatic.
- › Surgical indication disputes — Whether the spinal surgery that preceded the PLSS was clinically indicated — supported by appropriate clinical findings, imaging, and a documented failure of conservative care — is a recurring issue in both malpractice matters (where unnecessary surgery is alleged) and personal injury matters (where the defense argues that surgery was performed for a pre-existing condition rather than the accident). This question is within the spine surgery expert's scope, not the pain management expert's scope, but it affects the framework within which post-surgical pain management opinions are rendered.
- › Medical necessity of post-surgical treatment — Insurers and defense counsel frequently dispute the necessity of post-surgical pain management based on the volume of procedures, the adequacy of documentation, the relationship between procedures and documented clinical findings, or the appropriateness of escalation to SCS. These disputes arise both in pre-authorization contexts and in post-hoc defense review of past treatment.
- › SCS necessity disputes — Whether the clinical record supports SCS implantation — through documented indication, adequate conservative care trial, completed psychological screening, and a successful trial stimulation result — is the most significant individual issue in high-value PLSS cases. The adequacy of each element of the pre-implant evaluation is reviewed in detail in SCS necessity disputes.
- › Future care disputes — Defense review of plaintiff life care plans addresses whether proposed pain management items are clinically supported by the documented post-surgical course, whether SCS is a reasonable projection given the current clinical trajectory, whether projected frequencies and durations are consistent with clinical guidelines, and whether costs reflect current market pricing rather than published retail rates.
- › Pre-existing degenerative disease and apportionment — Degenerative disc disease and facet arthrosis are common findings in the adult spinal column, and their presence on pre-surgical imaging does not establish that the post-surgical pain is unrelated to the subject accident. The apportionment analysis must address whether the accident produced new injury or materially accelerated the pre-existing degenerative process, and what proportion of the current pain and functional limitation is attributable to accident-related pathology versus natural degenerative progression.
- › Functional impairment — The functional impact of post-laminectomy syndrome — on ambulation, sitting tolerance, vocational capacity, and activities of daily living — is frequently contested. Expert review addresses whether the functional limitations documented in the treating record are consistent with the pain syndrome and clinical findings, and whether the treating documentation adequately captures functional status over time. For a detailed discussion of how these findings translate into non-economic damages evidence, see the article on clinical methodology for pain and functional impairment.
Personal Injury Case Analysis
Motor vehicle collisions are the most common personal injury mechanism producing post-laminectomy syndrome in the litigation context. High-energy impacts producing herniated discs with significant nerve root compression — particularly at C5–C6, C6–C7, L4–L5, or L5–S1 — create a clinical pathway from accident to surgery to persistent post-surgical pain that is among the most common and highest-value damages trajectories in personal injury practice. The causation analysis for this pathway operates at three levels: whether the collision produced the disc herniation that required surgery; whether the surgery was clinically indicated; and whether the post-laminectomy syndrome is a foreseeable consequence of the surgery performed. When the disc herniation is central and severe enough to cause cauda equina syndrome requiring emergency decompression, the post-surgical pain analysis incorporates both the post-laminectomy syndrome framework and the distinct neuropathic sequelae — including bilateral radicular pain and perineal involvement from sacral nerve root injury — specific to cauda equina nerve root compression.
Pre-existing degenerative spinal disease is the most common complicating factor in personal injury PLSS cases. Degenerative disc disease and facet arthrosis are present in the majority of adults over forty and may be visible on pre-accident imaging if it exists, or inferred from post-accident imaging that shows advanced changes inconsistent with acute injury. The defense frequently argues that pre-existing degeneration — not the subject accident — caused the need for surgery and the resulting post-surgical pain syndrome. Expert causation analysis addresses this argument directly: the question is not whether degeneration existed, but whether the accident caused new structural injury, materially aggravated a symptomatic pre-existing condition, or accelerated an asymptomatic degenerative process to become clinically symptomatic requiring surgery. For a physician's methodology on distinguishing pre-existing degeneration from incident-related aggravation, see the article on pre-existing degeneration vs. aggravation in spine injury cases.
Future medical care projections in personal injury PLSS matters should account for the full anticipated treatment trajectory — ongoing pharmacological management, periodic interventional procedures, and in appropriate cases the costs of spinal cord stimulation including trial, permanent implantation, battery replacement cycles, and programming. When adjacent segment disease is anticipated based on the level and extent of fusion surgery performed, the potential for future surgery at adjacent levels is also a recognized future care consideration. Each component requires clinical support from the documented treatment record rather than generic template assumptions. Future medical care review for PLSS cases is grounded in the specific clinical course and the current treatment status — not in standardized life care plan templates.
Medical Malpractice Analysis
Malpractice matters involving post-laminectomy syndrome arise from post-surgical pain management failures rather than surgical errors — those are addressed by spine surgeon experts. Expert review in PLSS malpractice matters addresses whether the post-operative pain management provided met the standard of care for a reasonably competent pain management physician encountering a patient with persistent post-surgical spinal pain.
- › Failure to refer post-surgical patients to pain management — A spine surgeon managing a post-operative patient with persistent pain beyond the expected recovery timeframe has an obligation to consider referral to pain management. Failure to refer — or a significant delay in referral — can constitute a standard of care deviation when the patient has persistent neuropathic or mechanical post-surgical pain that is not responding to routine post-operative analgesic management. The appropriate referral window depends on the specific post-surgical presentation, but persistent radicular or neuropathic pain beyond three to six months post-surgery that has not been evaluated by a pain management specialist is commonly identified as a delayed-referral concern.
- › Inadequate post-surgical pain management evaluation — A pain management physician who assumes care of a PLSS patient without obtaining operative reports, post-surgical imaging, and a complete pre-surgical history cannot perform an adequate evaluation of the pain generators present. Treating without reviewing the operative record — and therefore without knowing what was done, what was found, and what was changed — is an evaluation standard of care issue. The operative report is essential to understanding the anatomy, the surgical findings, and the basis for the current pain pattern.
- › SCS complications and selection errors — Malpractice claims specific to SCS implantation for PLSS — including device complications, selection errors, and trial documentation failures — are addressed within the spinal cord stimulation expert review framework. These include the full range of SCS-specific standard of care issues: inadequate pre-implant evaluation, absence of psychological screening, inadequate trial documentation, and technical complications from lead placement.
- › Opioid management failures — Long-term opioid therapy for PLSS without appropriate monitoring, without prescription monitoring program compliance, or without documented reassessment of treatment goals may form the basis of claims where adverse outcomes — including overdose, addiction, or functional decline — are alleged to be consequences of prescribing below the applicable standard of care.
Expert review is specific to pain management and anesthesiology. Opinions on neurosurgical technique, spinal fusion standard of care, surgical indication, or post-operative surgical management are outside this scope and require a spine surgeon expert. The retaining attorney should identify whether pain management standard of care, surgical standard of care, or both are at issue, and retain appropriately scoped experts for each.
Future Medical Care Review
Future medical care for post-laminectomy syndrome is one of the most complex and high-value components of damages analysis in spinal injury litigation. The pain management component of future care must be grounded in the documented clinical course and current treatment status, and must account for the range of pain generators that may require treatment over the patient's lifetime.
- › Pharmacological management — Ongoing medication management for PLSS is a recognized long-term cost. Projected medications should reflect those currently in use with documented benefit, at current dosing, with current market pricing. Speculative projections of future medications not supported by the current treatment course are subject to challenge.
- › Interventional procedures — Periodic epidural steroid injections, medial branch blocks, and RFA cycles form a recognized recurring cost structure for patients with ongoing post-surgical radicular and facet-mediated pain. The frequency and cost of each procedure should be based on the documented treatment history and the treating physician's recommendations, not generic templates. Projected RFA cycles should account for the nerve regeneration timeline and the cost of confirmatory blocks preceding each ablation cycle.
- › Spinal cord stimulation — Where the clinical trajectory supports future SCS, the projection should include: the trial stimulation procedure; the permanent implantation cost with device-specific documentation; battery replacement at intervals consistent with the device type (rechargeable vs. non-rechargeable); revision procedures at published complication rates; and ongoing programming visits. The basis for projecting SCS — specifically, whether the clinical record supports its medical necessity — must be addressed before including it as a future care line item.
- › Adjacent segment and revision surgery considerations — When the patient has undergone spinal fusion and the clinical and imaging record suggests progressive adjacent segment changes, the potential for future adjacent segment surgery may be a legitimate future care element. This projection requires a spine surgeon's opinion on surgical likelihood and timing; the pain management expert's contribution is the post-surgical pain management component that would follow any such future procedure.
- › Defense review of life care plans — Defense review of a plaintiff's PLSS future care projection addresses whether each proposed item is clinically supported by the documented post-surgical course, whether SCS necessity is established by the available record, whether frequencies and durations are grounded in clinical prognosis, and whether costs reflect the plaintiff's geographic treatment market rather than national list prices.
Future medical care review for PLSS cases can be structured as a standalone engagement or combined with causation analysis. Contact Expert Medical Services LLC to discuss the scope and available records.
Expert Witness Review Process
Post-laminectomy syndrome cases require review of a defined set of records to support a complete medical-legal opinion. The scope of records needed depends on whether the engagement addresses causation, medical necessity, standard of care, future care, or a combination, and is defined in consultation with retaining counsel. Typical records include:
- › Operative reports — All operative reports from spinal surgeries performed in connection with the case, including the primary procedure and any subsequent revisions, fusion extensions, or adjacent-level procedures; intraoperative findings; and post-operative orders
- › Pre-surgical clinical records — The treating records from the period between the subject event and the surgical decision, documenting symptom onset, clinical findings, the conservative treatment course, and the basis for the decision to proceed with surgery
- › Imaging studies — Pre-surgical and post-surgical MRI and CT scans of the relevant spinal levels, with reports; post-surgical imaging documenting the surgical result, hardware position, fusion status, and any evolving adjacent segment or recurrent pathology
- › Complete treating pain management records — Initial evaluation, follow-up clinical notes, pre-procedure assessments, procedure reports, post-procedure response documentation, and pharmacological management notes from the beginning of the pain management relationship through the most recent encounter
- › Physical and occupational therapy records — Rehabilitation documentation from both the pre-surgical and post-surgical periods, documenting treatment approach, patient response, and functional outcome measures
- › SCS-related records (where applicable) — Pre-implant psychological evaluation report; trial stimulation records including pre-trial and post-trial pain scores; permanent implant operative report and device documentation; post-implant programming records and follow-up notes
- › Prior treating records — Records predating the subject event to establish baseline spinal health, prior spinal treatment history, and any pre-existing conditions relevant to causation or apportionment
- › Billing records and insurance correspondence — Itemized billing and pre-authorization records where medical necessity disputes with payers are at issue
- › Deposition testimony — Testimony of the treating pain management physician, the spine surgeon, and any retained experts addressing the diagnosis, causation, or treatment course; as well as claimant testimony addressing symptom history and functional limitations
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. Engagements addressing causation, causation analysis, standard of care, and future medical care projections can be structured separately or together within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Spinal Cord Stimulation
SCS is the primary advanced treatment for PLSS — medical necessity, cost projections, and expert testimony.
CRPS Expert Witness
CRPS Type II may follow spinal surgery — diagnosis, causation, Budapest Criteria, and future care.
Radiofrequency Ablation
Expert review of RFA for facet-mediated pain components in post-surgical spinal pain litigation.
Medial Branch Block
Expert review of MBB and the diagnostic pathway to RFA for facet pain following spinal surgery.
Epidural Steroid Injections
Expert evaluation of ESI for post-surgical radicular pain — medical necessity, standard of care, and future care projections.
Future Medical Care Review
Projecting SCS, interventional procedures, and long-term pharmacological care costs following spinal surgery.
Causation Analysis
Establishing whether the subject incident contributed to the spinal condition requiring surgery.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California spinal surgery matters.
Peripheral Nerve Injury
Nerve root injury and traumatic neuropathy that may complicate post-surgical spinal pain.
Arizona Pain Management Expert Witness
Post-laminectomy syndrome expert review for Arizona personal injury litigation.
Florida Pain Management Expert Witness
Post-laminectomy syndrome expert review for Florida personal injury and medical malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for post-laminectomy pain interventions including neuromodulation and intrathecal therapy.
Standard of Care Analysis
Standard of care analysis for post-surgical spinal pain management and escalation of interventional treatment.
FAQ
Post-Laminectomy Syndrome — Common Attorney Questions
- Post-laminectomy syndrome is persistent or recurrent spinal pain that continues following spinal surgery — including laminectomy, discectomy, spinal fusion, or combined procedures — in the absence of recognized intraoperative complications. The term applies when a patient who undergoes spinal surgery for disc herniation, spinal stenosis, or instability continues to experience significant pain after surgery, or when pain initially improves and then returns. It is not a judgment on the quality of the surgical procedure. It reflects the clinical reality that spinal pain has multiple potential generators, that surgery addresses structural pathology but does not uniformly resolve the underlying neurobiological pain state, and that some patients develop new or secondary pain mechanisms following the surgical intervention itself. Post-laminectomy syndrome is the most common indication for spinal cord stimulation implantation in the United States.
- Persistent post-surgical spinal pain can arise from several distinct mechanisms that may occur alone or in combination. Epidural fibrosis — the formation of scar tissue around nerve roots following surgery — is one of the most frequently identified contributors and can produce radicular pain by mechanically tethering or compressing the affected nerve root. Recurrent disc herniation at the same level that was operated on is a distinct structural cause that produces a clinical picture similar to the original presentation. Adjacent segment disease refers to accelerated degenerative change at spinal levels immediately above or below a fusion construct, a well-documented biomechanical consequence of altered load distribution after fusion surgery. Failed spinal fusion — pseudarthrosis — produces ongoing instability and mechanical pain because the intended bony union was not achieved. Hardware-related pain from implanted instrumentation — pedicle screws, rods, or interbody devices — can produce mechanical and inflammatory pain at the implant site. Neuropathic central sensitization, in which the pain system itself has undergone neuroplastic changes from prolonged pre- and post-surgical pain signaling, can perpetuate pain independent of any ongoing structural source.
- Causation review in post-laminectomy syndrome cases operates on two levels. The first level addresses whether the subject incident — a motor vehicle collision, a workplace injury, or another traumatic event — produced the underlying spinal injury that required surgery. This analysis reviews the temporal relationship between the event and symptom onset, the mechanism of injury and its anatomical consistency with the surgical pathology, the pre-accident medical history, and the clinical documentation from the period between the event and the surgical decision. The second level addresses whether the post-laminectomy syndrome — the persistent post-surgical pain — is a recognized and foreseeable consequence of that surgery. Post-laminectomy syndrome is a documented outcome of spinal surgery and does not require a distinct causation analysis from the surgery itself when the surgery is established as causally related to the traumatic event. Cases involving pre-existing degenerative spinal disease require a specific analysis of whether the surgery was performed to address traumatic injury, aggravated pre-existing pathology, or primarily pre-existing disease.
- Post-laminectomy syndrome is a clinical pain diagnosis that describes persistent pain after spine surgery — it is not equivalent to a surgical complication. A recognized surgical complication involves a discrete, identifiable adverse event — nerve root injury from surgical trauma, dural tear with cerebrospinal fluid leak, wrong-level surgery, infection requiring hardware removal, or vascular injury. Post-laminectomy syndrome, by contrast, reflects the natural history of post-surgical spinal pain in a subset of patients and does not imply any departure from the surgical standard of care. The distinction is important in the litigation context because the causation analysis, the standard of care framework, and the damages structure differ between a PLSS case and a surgical complication case. In malpractice matters involving spinal surgery, expert review may need to address both the surgical standard of care and the post-operative pain management standard of care — these are separate questions requiring separate expertise.
- Spinal cord stimulation is considered for post-laminectomy syndrome when the persistent post-surgical pain is refractory to an adequate trial of conservative and conventional interventional management — including pharmacological treatment with neuropathic agents, epidural steroid injections, physical therapy, and other modalities appropriate to the specific pain pattern. Post-laminectomy syndrome is the most common overall indication for SCS implantation in the United States, and the evidence base supporting SCS for PLSS is among the strongest in the neuromodulation literature. The evaluation for SCS candidacy requires a documented treatment history demonstrating failure of appropriate conservative care, a psychological screening evaluation, and a successful SCS trial demonstrating adequate pain relief before permanent implantation. In personal injury litigation, when a traumatic event leads to spinal surgery and persistent post-surgical pain develops, the potential future need for SCS becomes a recurring future care element that can significantly affect damages calculations. Medical necessity review addresses whether the post-surgical pain pattern is consistent with a recognized SCS indication and whether the clinical record supports the progression to neuromodulation.
- Adjacent segment disease refers to accelerated degenerative change at spinal levels immediately above or below a spinal fusion construct. Fusion surgery alters the biomechanics of the spinal column by eliminating motion at the fused level, which transfers increased mechanical load to the adjacent unfused segments. Over time, this altered load distribution can accelerate disc degeneration, facet arthropathy, and stenosis at the adjacent levels — producing a new pain generator that was not the primary target of the original surgery. Adjacent segment disease arises in litigation in several contexts. In personal injury cases, it is a recognized long-term sequela of fusion surgery that can affect future care projections when the original fusion was necessitated by a traumatic injury. In malpractice cases, it may be relevant when the indication for fusion surgery is disputed — specifically, whether fusion was clinically necessary or whether a less extensive procedure would have addressed the pathology without producing adjacent segment consequences. Expert review addresses whether adjacent segment disease is present, whether it is a foreseeable consequence of the prior surgery, and whether it requires additional treatment.
- The standard of care for post-surgical pain management addresses the obligations of the pain management physician who assumes care of a patient with persistent post-surgical spinal pain. Core elements include a complete initial evaluation that characterizes the specific pain generators present — distinguishing between radicular, axial, neuropathic, and mechanical pain components — and a treatment plan that is appropriately matched to those generators. Failure to complete an adequate evaluation before initiating interventional procedures, prescribing opioids without an appropriate monitoring framework, progressing to advanced interventions such as SCS without completing a documented conservative care trial, or failing to recognize and address psychological comorbidities that affect treatment outcome are all standard of care considerations in post-surgical pain management. In malpractice matters arising from post-surgical pain management specifically — rather than from the surgery itself — these are the clinical standards against which the treating pain management physician's care is evaluated.
- Yes. When the clinical record supports a trajectory toward SCS — either because the treating physician has recommended it, because the conservative care trial has been completed without adequate relief, or because the documented clinical course is consistent with a PLSS pattern that typically requires neuromodulation — future SCS costs are a recognized component of personal injury damages analysis. A defensible future SCS projection for a PLSS patient should include: the trial stimulation procedure and its associated costs; the permanent implantation procedure with device-specific cost documentation; battery replacement cycles at intervals consistent with the device type (rechargeable vs. non-rechargeable); revision procedure allowances based on published hardware complication rates; and ongoing programming and device management visits. The aggregate cost of SCS over the patient's life expectancy is a significant damages component in high-value spinal injury cases, and it requires a physician opinion grounded in the clinical record to be defensible.
- Key records include: the complete treating pain management notes from post-surgical referral through the most current encounter; the operative report(s) from all spinal surgeries, including the original procedure and any revision or adjacent-level procedures; pre-surgical imaging documenting the pathology that led to surgery; post-surgical imaging documenting the surgical result and any evolving findings; the pre-operative clinical workup including any pre-surgical pain management records; physical therapy records from both pre- and post-surgical rehabilitation; billing records where treatment volume or cost is at issue; prior treating records predating the surgical episode to establish baseline spinal health; and, where SCS is at issue, the pre-implant psychological evaluation, trial stimulation records, and post-implant programming and follow-up documentation.
- Yes. Dr. Dardashti accepts post-laminectomy syndrome engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides. Review is available for causation analysis, treatment necessity and standard of care review, and future medical care projections — or for a defined subset of those issues based on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain Dr. Dardashti for a Post-Laminectomy Syndrome Case
Dr. Dardashti accepts post-laminectomy syndrome engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.