Nationwide Pain & Injury Medical Expert Witness
Spinal Cord Stimulation Expert Witness
Independent expert review of spinal cord stimulation trials, permanent implants, medical necessity, device complications, future medical care projections, and litigation issues in personal injury and medical malpractice matters.
Request AvailabilityCredentials & Qualifications
- Topic
- Spinal Cord Stimulation (SCS)
- Also Known As
- Neuromodulation, Dorsal Column Stimulation
- Primary Indications
- CRPS, Post-Laminectomy Syndrome, Refractory Neuropathic Pain
- Evaluation Areas
- Medical Necessity, Standard of Care, Causation, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Spinal Cord Stimulation in Litigation
Spinal cord stimulation is one of the highest-cost, highest-stakes interventional pain procedures in personal injury and medical malpractice litigation. In personal injury cases, SCS arises as a proposed future care item that can add hundreds of thousands of dollars to the damages calculation — or as a past treatment whose necessity and causal relationship to the subject incident is disputed. In medical malpractice cases, SCS arises when device complications, selection errors, or technical failures during implantation are alleged to have caused harm.
SCS litigation requires a pain management physician who can address the full clinical picture: whether the underlying condition justifies implantation, whether the required evaluation and trial were performed and documented, whether the trial result meets the clinical threshold for proceeding to permanent implantation, whether complications were the result of recognized risks or technical deviations, and what a defensible long-term cost projection for a patient requiring SCS looks like. These are pain management questions, and they require a board-certified pain management specialist to answer them.
What Is Spinal Cord Stimulation?
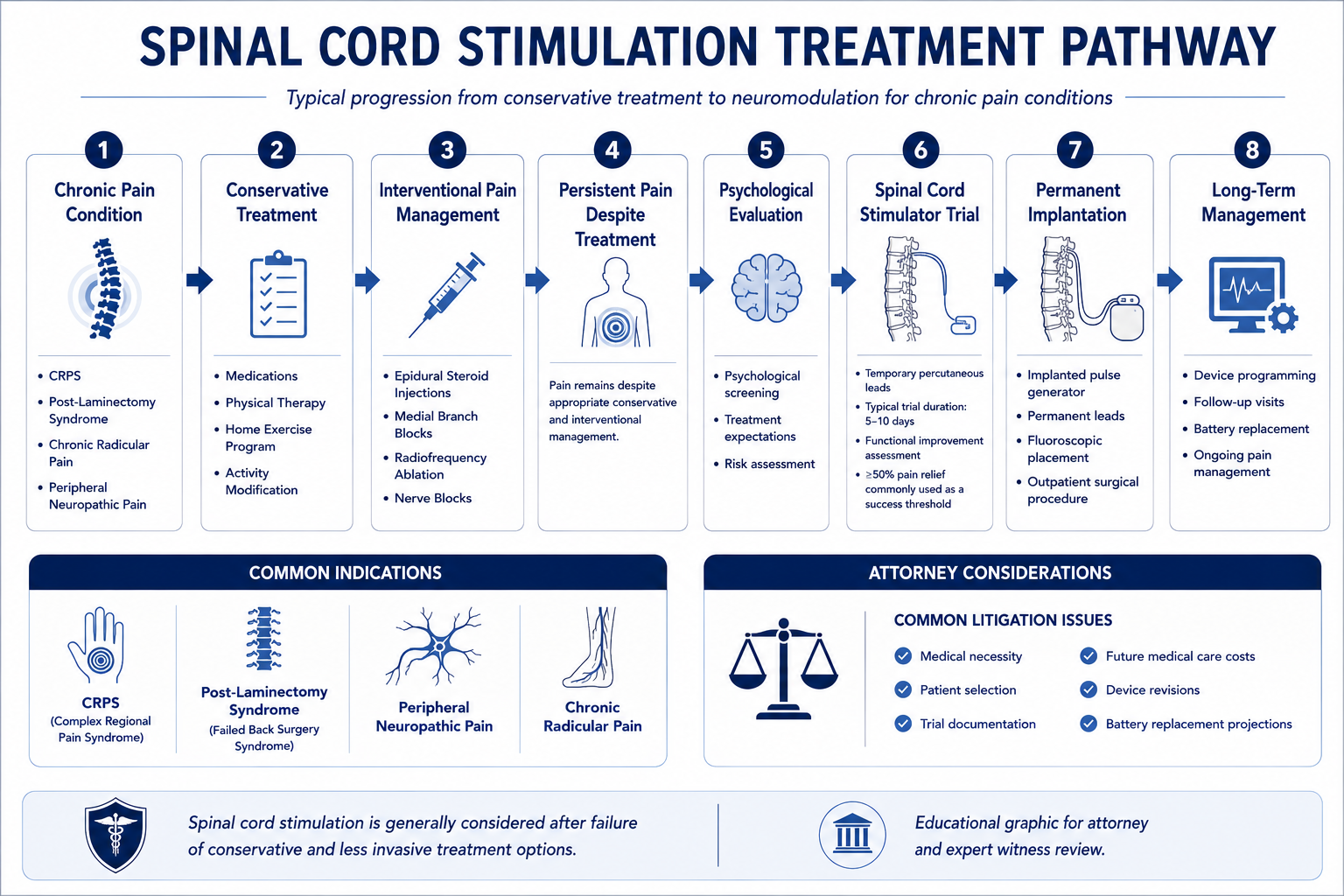
Spinal cord stimulation is a neuromodulation procedure in which an implanted pulse generator delivers electrical impulses through epidurally placed leads to the dorsal columns of the spinal cord. By delivering low-level electrical current to the dorsal horn and posterior column fibers, SCS modulates the transmission of pain signals ascending toward the brain — reducing perceived pain intensity without ablating nerve tissue and without the systemic effects of long-term opioid therapy.
The SCS system consists of three main components: epidural leads (percutaneous or surgical paddle), an implantable pulse generator (IPG) or rechargeable battery unit, and an external programmer used by the physician and patient to adjust stimulation parameters. Percutaneous leads are placed through epidural needles under fluoroscopic guidance; paddle leads require a more invasive surgical approach through a small laminotomy or laminectomy. The choice of lead type and placement level is determined by the target pain distribution — cervical leads for upper extremity or neck pain, thoracic leads for lower extremity and axial back pain.
Traditional SCS delivers paresthesia — a tingling sensation — in the distribution of the pain, which the patient perceives as covering or replacing the pain. Newer waveform technologies — including high-frequency stimulation (10 kHz), burst stimulation, and closed-loop adaptive stimulation — produce pain relief without paresthesia and are associated with different programming requirements and evidence profiles. The distinctions between these modalities are relevant to both the clinical standard of care and the device cost structure in future care projections.
Unlike ablative procedures, SCS is reversible. The device can be turned off, reprogrammed, or surgically explanted. Reversibility is both a clinical advantage and a medico-legal distinction — patients who do not achieve adequate relief with SCS, or who experience device complications, may have the system revised or removed. The cost and clinical implications of revision and explantation are components of expert review in SCS complication and failure cases.
Trial Stimulation
The SCS trial is a mandatory preliminary phase in which temporary leads are placed epidurally and connected to an external pulse generator for a defined trial period — typically seven to ten days — during which the patient evaluates pain relief in their normal environment before permanent implantation is authorized. The trial serves two clinical and regulatory functions: it confirms that SCS produces adequate pain relief for this specific patient, and it allows the patient to experience the sensation and practical implications of the therapy before committing to permanent implantation.
A successful trial is generally defined as a reduction in pain intensity of at least 50%, assessed through validated pain outcome measures obtained both immediately before the trial and during the trial period. Some clinical protocols and payer criteria additionally require functional improvement or reduction in analgesic consumption as secondary success measures. At the conclusion of the trial, the temporary lead is removed and the clinical documentation of trial results — including pre-trial and post-trial pain scores — forms the evidentiary basis for permanent implant authorization.
Documentation of the trial result is the pivotal record in SCS medical necessity review. The treating physician should document: baseline pain scores using a validated instrument (VAS or NRS) before trial placement; post-trial pain scores using the same instrument at conclusion; percentage improvement in pain; any functional changes observed during the trial; patient and physician assessment of trial success; and the clinical basis for the decision to proceed or not proceed to permanent implantation. For the complete clinical evaluation framework — examination, imaging, validated instruments, and functional assessment — that underlies a pain management physician's opinion on functional impairment and SCS necessity, see the article on how pain management experts objectively evaluate pain. For a detailed framework governing medical necessity analysis for spinal cord stimulators specifically, see the article on how pain management experts evaluate medical necessity for spinal cord stimulators.
- › Missing trial documentation — Permanent SCS implantation without documented trial results is a recognized medical necessity and standard of care issue. The trial is not a formality — it is the clinical mechanism by which patient response is confirmed before permanent device implantation.
- › Inadequate trial duration — Trials that are terminated prematurely — before the patient has had adequate time to evaluate the therapy in their normal daily activities — may not provide a reliable basis for proceeding to permanent implantation. The standard trial duration of seven to ten days is designed to allow assessment across different activity levels and times of day.
- › Trial vs. trial failure — When the SCS trial does not produce the required percentage improvement in pain, permanent implantation is not clinically supported. Implantation after a documented failed trial — or without any trial — is a recurring standard of care issue in SCS malpractice matters.
Permanent Implantation
Permanent SCS implantation follows a successful trial and involves surgical placement of permanent epidural leads and an implantable pulse generator in a subcutaneous pocket, typically in the abdomen or buttock. The permanent implant procedure is substantially more invasive than the trial and carries a distinct risk profile — including risks of lead migration, hardware failure, infection, seroma or hematoma, and the need for future revision or replacement surgery. Informed consent for permanent implantation addresses these risks as well as the long-term maintenance implications of the device.
Patient selection for permanent SCS implantation requires evaluation of multiple clinical, psychological, and practical factors. The patient must have a diagnosis that falls within a recognized SCS indication, must have failed an adequate course of conservative treatment, must have undergone and passed a psychological screening evaluation, must have had a successful trial, and must be an appropriate surgical candidate from a medical standpoint. Failure to complete any component of this evaluation sequence before proceeding to permanent implantation is a standard of care concern.
The choice between non-rechargeable and rechargeable IPG systems affects both the short-term surgical approach and the long-term cost and maintenance structure. Non-rechargeable systems require more frequent battery replacement surgeries — typically every two to five years — but do not require the patient to charge the device regularly. Rechargeable systems require daily or weekly charging by the patient but have longer projected battery life before surgical replacement is required. In future care projections, the distinction between device types materially affects the projected replacement frequency and aggregate cost over the patient's life expectancy.
Medical Necessity Analysis
Medical necessity for spinal cord stimulation is evaluated against the clinical record and applicable treatment guidelines. A supported indication generally requires: a diagnosis within a recognized SCS indication category; a documented history of failure of conservative treatment to provide adequate relief; completion of pre-implant psychological evaluation; a successful trial stimulation with contemporaneous documentation; and a treating physician's clinical rationale connecting the patient's condition to the proposed device.
CRPS is one of the most frequently encountered SCS indications in personal injury litigation. Randomized controlled evidence supports SCS for CRPS when the condition is refractory to conventional pain management — including physical therapy, sympathetically targeted procedures, and pharmacological management. When CRPS arises from a traumatic accident and evolves to the point where SCS is indicated, the cost of the implant and its long-term maintenance becomes a significant component of personal injury damages.
Post-laminectomy syndrome — persistent spinal pain following surgery — is the most common overall indication for SCS implantation in the United States. When a traumatic event leads to spinal surgery and persistent post-surgical pain develops, the potential future need for SCS becomes a recurring future care issue. Necessity review addresses whether the post-surgical pain pattern is consistent with a recognized SCS indication, whether the clinical record documents failure of appropriate conservative and interventional post-surgical management, and whether the treating physician's recommendation is supported by the available record.
Refractory peripheral neuropathic pain following nerve injury — including traumatic mononeuropathy — is an additional recognized SCS indication when the neuropathic pain is refractory to pharmacological and interventional management. The clinical basis for SCS in this context requires electrodiagnostic documentation of the nerve injury, evidence of persistent pain refractory to conservative management, and a pain pattern consistent with the neuropathic distribution of the injured nerve.
Failure of conservative care is a threshold element of the necessity analysis. SCS is an advanced pain management option, not a first-line therapy. Procedural timelines that show SCS implantation without evidence of an adequate prior treatment course — including pharmacological management, physical therapy, and appropriate interventional pain procedures — may face medical necessity challenges regardless of the diagnosis. The adequacy of the conservative treatment trial is evaluated against the specific diagnosis and the recognized treatment ladder for that condition. When anatomical factors, prior spinal surgery, or patient-specific considerations make SCS technically unfeasible — or when SCS fails after an adequate documented trial — intrathecal drug delivery represents an alternative implantable neuromodulation pathway within the same advanced pain management spectrum.
Standard of Care Considerations
The standard of care for SCS implantation reflects the practice of a reasonably competent board-certified or board-eligible pain management physician performing the procedure in accordance with current professional guidelines. Core elements include appropriate patient selection through a multidisciplinary evaluation, completion of the required pre-implant assessment sequence, performance of an adequate trial, technically appropriate implant procedure, and ongoing post-implant management.
- › Psychological screening — Pre-implant psychological evaluation by a qualified mental health provider is a standard of care requirement for SCS implantation. The evaluation assesses psychological factors that may affect treatment outcome — including untreated depression, somatization, active substance use disorder, secondary gain issues, and unrealistic expectations. Implantation without completed psychological screening is a recognized standard of care deviation and a common source of medical necessity disputes with payers.
- › Trial stimulation requirement — Proceeding to permanent implantation without a completed and documented trial is below the standard of care. The trial is not a payer formality — it is a clinical requirement designed to verify patient response before a more invasive and costly permanent procedure is performed.
- › Documented trial result — The trial result must be documented contemporaneously with validated outcome measures. A physician's retrospective characterization of the trial as successful, without contemporaneous pain score documentation, does not meet the evidentiary and clinical standard. This documentation gap is a recurring issue in SCS necessity disputes.
- › Fluoroscopic guidance for lead placement — Lead placement during both the trial and permanent implant procedures is performed under fluoroscopic guidance to confirm epidural entry, lead position, and coverage pattern. Failure to use image guidance or to document radiographic confirmation of lead position is relevant to standard of care review in lead-related complication cases.
- › Intraoperative testing — Intraoperative stimulation testing during permanent lead placement (awake or under light sedation) or intraoperative electrophysiological monitoring confirms that paresthesia coverage matches the patient's pain distribution. Documented intraoperative confirmation is the standard practice to verify appropriate lead placement before tunneling and IPG implantation.
- › Post-implant programming and follow-up — Appropriate SCS management includes post-implant programming visits to optimize stimulation parameters, monitoring of device function, and clinical follow-up to assess ongoing pain relief and functional status. Inadequate post-implant follow-up that results in suboptimal outcomes or missed complications may be relevant to standard of care review.
Common Litigation Issues
SCS cases present a defined set of litigation issues that recur across personal injury and medical malpractice contexts. The issues cluster around three areas: whether SCS was medically necessary and properly performed, whether device complications resulted from standard risks or technical deviations, and what the appropriate future cost projection looks like.
- › Medical necessity disputes — Insurers and defense counsel frequently dispute SCS necessity based on failure to document adequate conservative care, absence of psychological screening, inadequate trial documentation, or the treating physician's failure to address pre-existing conditions in the necessity analysis. These disputes arise both in pre-authorization denials and in post-hoc defense review of past treatment.
- › Failed implant claims — When SCS fails to produce adequate ongoing relief after permanent implantation — despite an initially documented successful trial — the patient may require revision lead placement, device reprogramming, or ultimately explantation. Claims involving failed implants address whether the trial result truly supported permanent implantation, whether post-implant programming was adequate, and whether device failure was the result of a technical defect, a hardware complication, or an appropriate failure of therapy in a non-responder.
- › Lead migration disputes — Lead migration — displacement of the stimulation lead from the target epidural position — is a recognized and common hardware complication of SCS that can result in loss of pain coverage or unwanted stimulation patterns. Claims addressing lead migration raise questions about whether the original lead placement was adequate, whether the migration resulted from a technical error or from a recognized positional risk, and whether the physician's response to migration (reprogramming vs. surgical revision) was appropriate.
- › Infection requiring explantation — Device infection following SCS implantation is a serious complication that may require complete hardware removal — explantation — followed by a course of antibiotics before reimplantation can be considered. Claims address sterile technique, wound care instructions, recognition of early infection signs, and the adequacy of the clinical response once infection was identified. Explantation represents a significant clinical harm because it deprives the patient of a therapy that was working and may require the full trial-to-permanent-implant sequence to be repeated.
- › Causation disputes — Whether the underlying condition requiring SCS arose from the subject accident, aggravated a pre-existing condition, or was unrelated to the claimed injury is a central question in personal injury matters where SCS is proposed as future care. The causation analysis for the underlying SCS indication is distinct from but clinically related to the medical necessity analysis for the device itself. Where spinal degeneration is present, distinguishing pre-existing pathology from incident-related aggravation is a foundational analytical step — see the article on pre-existing degeneration vs. aggravation in spine injury cases.
- › Future care cost disputes — Defense review of plaintiff SCS future care projections focuses on whether the projected replacement frequency is consistent with the device type, whether costs reflect current market pricing, whether the duration of SCS need is supported by the clinical record, and whether alternative or less costly management options are available that would provide similar outcomes.
Personal Injury Case Analysis
In personal injury litigation, SCS most commonly arises as a proposed future care item — a treatment that the injured plaintiff will require in the future as a result of the subject accident. The two most common pathways to future SCS in personal injury cases are: (1) CRPS developing after a traumatic injury, with SCS indicated when the condition becomes refractory to conventional management; and (2) spinal surgery for traumatic disc injury followed by post-laminectomy syndrome, where persistent post-surgical pain becomes a candidate for neuromodulation.
Causation review in the SCS context operates on two levels. At the first level, causation analysis addresses whether the underlying condition — the CRPS or the post-laminectomy syndrome — is attributable to the subject accident. At the second level, medical necessity review addresses whether that underlying condition, once established as causally related, justifies SCS implantation based on the clinical record. These are distinct analyses that are best structured clearly for the fact-finder: causation establishes the link to the accident; necessity establishes that SCS is the appropriate treatment for the resulting condition.
Future SCS projections in personal injury cases should be grounded in the specific clinical trajectory documented in the treating records. An expert who proposes future SCS in a case where the treating physician has not discussed or recommended SCS, where the patient has not completed a conservative care trial, or where the underlying condition has not reached the clinical threshold for SCS consideration is vulnerable to challenge on both necessity and causation grounds. Conversely, a case where the treating physician has already documented SCS as the recommended next treatment step provides substantially stronger support for a future care projection.
High-value SCS future care projections may include: the trial stimulation procedure; the permanent implantation procedure; battery replacement cycles at intervals consistent with the device type over the patient's life expectancy; revision procedures at a rate consistent with the published hardware complication literature; ongoing programming visits; and the cost of medication management during any periods when SCS provides incomplete coverage. Each of these components should be separately itemized and priced to the plaintiff's geographic market in a comprehensive future medical care review.
Medical Malpractice Analysis
Malpractice claims involving spinal cord stimulation arise from patient selection errors, inadequate pre-implant evaluation, technical complications during implantation or revision, and post-implant management failures. Expert review addresses whether the care provided by the treating pain management physician or implanting surgeon met the applicable standard of care for a board-certified specialist performing SCS in the relevant clinical context.
- › Implantation without required pre-implant evaluation — Proceeding to permanent implantation without completed psychological screening, without a documented successful trial, or without an established indication within recognized SCS criteria is a departure from the clinical standard. These are threshold requirements, not procedural technicalities.
- › Spinal cord or nerve root injury during implantation — Lead placement during SCS trial or permanent implantation carries a small but recognized risk of spinal cord or nerve root injury from needle trauma, lead trauma, or epidural hematoma. The standard of care requires fluoroscopic guidance, careful needle and lead advancement technique, and post-procedure neurological monitoring. Claims addressing neurological injury evaluate whether the standard precautions were followed and documented.
- › Epidural hematoma — Epidural hematoma following SCS lead placement is a rare but serious complication that can result in cord compression and permanent neurological injury if not recognized and treated promptly. The standard of care requires pre-procedure review of anticoagulation status, appropriate anticoagulation management, and post-procedure monitoring for neurological signs. Claims address both the technical conduct of the procedure and the adequacy of post-procedure observation.
- › Infection leading to explantation — Device infection requiring explantation represents a major clinical harm. Malpractice claims address: whether sterile technique was maintained during the implant procedure; whether the patient received appropriate post-procedure wound care instructions; whether early infection signs were recognized and acted upon promptly; and whether explantation was necessary or whether the infection could have been managed with the device in place. Failed recognition of early infection resulting in delayed treatment may be a basis for claims addressing the outcome of the infection course.
- › Failure to manage lead migration — Lead migration is a common hardware complication that results in loss of pain coverage or unwanted stimulation. While migration is a recognized and accepted risk of percutaneous SCS leads, the physician's response — appropriate reprogramming attempts followed by surgical revision when indicated — is subject to standard of care review. Failure to address documented lead migration that results in prolonged inadequate pain control may be relevant to the standard of post-implant management.
- › Patient selection errors — Implanting SCS in patients with active untreated psychiatric conditions, active substance use disorders, or conditions that are contraindications to implantable devices may form the basis of a claim where the outcome is adverse and the pre-implant screening records do not reflect awareness of these factors. The psychological screening requirement exists specifically to identify these risk factors before implantation.
Expert review is within the scope of pain management and anesthesiology. Opinions on neurosurgical technique in cases involving surgical complications that require neurosurgical expertise are outside this scope. The retaining attorney should identify the specific standard of care questions to be addressed at the time of engagement initiation.
Future Medical Care Review
Spinal cord stimulation is one of the most cost-intensive future care items in personal injury damages analysis. The aggregate cost of trial stimulation, permanent implantation, battery replacement cycles, revision procedures, programming visits, and associated medication management over a patient's life expectancy can reach six figures or more — making SCS future care a significant driver of damages in high-value personal injury and catastrophic injury cases. A defensible future care projection requires both clinical and economic accuracy.
- › Trial stimulation costs — Future SCS projections in cases where SCS has not yet been implanted should include the trial procedure — lead placement, external pulse generator rental, and the removal procedure at conclusion of the trial. Trial costs are real costs in the treatment pathway and should not be omitted from future care calculations.
- › Permanent implantation — The initial permanent implant procedure is the largest single cost component, comprising the device cost, the surgical facility fee, the implanting physician fee, and any anesthesia charges. Device costs vary by manufacturer and model — high-frequency and rechargeable systems typically carry higher device costs than conventional non-rechargeable systems. Future care projections should identify the device type assumed and provide cost documentation consistent with current market pricing in the plaintiff's geographic area.
- › Battery replacement frequency and cost — The projected IPG battery replacement interval depends on the device type: non-rechargeable conventional systems typically require replacement every two to five years; high-frequency non-rechargeable systems may require more frequent replacement due to higher energy consumption; rechargeable systems have longer projected battery life before surgical replacement but still require eventual replacement. The projected number of replacement surgeries over the plaintiff's life expectancy, multiplied by the per-replacement cost, is a major driver of the aggregate SCS future care total.
- › Revision procedures — Hardware complication rates — including lead migration and lead fracture — are published in the SCS literature and justify inclusion of a projected revision rate in future care analyses. The frequency and cost of revision surgery should be based on published complication data rather than assumed to be zero.
- › Programming and device management — Ongoing SCS management includes post-implant programming visits at intervals defined by device stability and patient needs, typically more frequent in the first year after implantation and less frequent thereafter. Annual or biannual device management visits are a recognized recurring cost component of SCS maintenance.
- › Defense review of life care plans — Defense review of a plaintiff's SCS future care projection addresses: whether SCS necessity is clinically supported by the documented treatment course; whether the device type and replacement frequency assumed in the projection are appropriate for the clinical scenario; whether costs reflect the plaintiff's treating market rather than published retail figures; and whether the duration of SCS need is grounded in the clinical record rather than assumed for the full life expectancy without clinical support.
Future medical care review for SCS cases can be structured as a standalone engagement or combined with causation analysis. Contact Expert Medical Services LLC to discuss scope and available records.
Expert Witness Review Process
Spinal cord stimulation cases require review of a defined set of records to support a complete medical-legal opinion. The specific records relevant to the engagement depend on the scope — medical necessity, standard of care, causation of the underlying condition, or future medical care — and are defined in consultation with retaining counsel. Typical records include:
- › Complete treating pain management records — Initial evaluation, follow-up clinical notes, pre-procedure assessments, and post-procedure response documentation from the beginning of the pain management relationship through the most recent visit
- › Pre-implant psychological evaluation — The screening report addressing psychiatric diagnoses, substance use history, psychosocial factors, and the evaluator's recommendation regarding SCS candidacy; essential for both necessity and standard of care review
- › Trial stimulation records — Trial procedure report, pre-trial pain outcome measures, post-trial pain outcome measures documenting percentage improvement, and the treating physician's documented assessment of trial success or failure
- › Implant operative reports and device records — Permanent implant operative report, device model and serial number documentation, lead placement fluoroscopy records, intraoperative testing documentation, and IPG model specifications
- › Post-implant programming records — Device programming visit notes documenting stimulation parameters, coverage mapping, ongoing pain scores, and any reprogramming rationale; relevant to both post-implant management standards and outcome assessment
- › Imaging studies — Pre-implant spinal imaging (MRI or CT) documenting the underlying condition, and post-implant imaging where lead position or hardware complications are at issue
- › Revision and complication records — Operative reports for any revision procedures, records of complication management, and any explantation documentation where device removal occurred
- › Prior treating physician records — Records predating the pain management relationship to establish the pre-injury baseline, prior treatment history, and absence or presence of pre-existing conditions at the relevant levels
- › Billing records and insurance authorization records — Itemized billing by procedure and service, pre-authorization requests, and payer decisions where a medical necessity dispute is at issue
- › Deposition testimony — Testimony of the treating pain management physician and implanting physician addressing clinical rationale, patient selection, procedural decisions, and post-implant management; as well as claimant testimony and testimony of any other retained experts addressing overlapping issues
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. Engagements addressing medical necessity, standard of care, causation, and future medical care can be structured separately or together within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
CRPS Expert Witness
CRPS is one of the primary SCS indications — diagnosis, causation, Budapest Criteria, and future care.
Post-Laminectomy Syndrome
Post-surgical spinal pain — the other primary SCS indication in personal injury litigation.
Peripheral Nerve Injury
Traumatic neuropathy and refractory neuropathic pain — a recognized SCS indication in complex cases.
Radiofrequency Ablation
Expert review of RFA medical necessity, standard of care, and future care in spinal pain litigation.
Medial Branch Block
Expert review of MBB and the diagnostic pathway from blocks to RFA to potential SCS escalation.
Future Medical Care Review
SCS trial, implant, battery replacement, and long-term programming cost projections for damages analysis.
Causation Analysis
Linking the subject incident to the underlying condition requiring spinal cord stimulation.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California SCS matters.
Amputation & Phantom Limb Pain
Phantom limb pain following amputation — SCS and peripheral nerve stimulation for refractory neuropathic pain.
Texas Pain Management Expert Witness
Spinal cord stimulation expert review for Texas personal injury and medical malpractice litigation.
Arizona Pain Management Expert Witness
Spinal cord stimulation expert review for Arizona personal injury litigation.
Florida Pain Management Expert Witness
Spinal cord stimulation expert review for Florida personal injury and medical malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for spinal cord stimulation — candidacy, trial documentation, and implant justification.
Standard of Care Analysis
Standard of care analysis for SCS trial, implant, and ongoing device management in spinal pain cases.
FAQ
Spinal Cord Stimulation — Common Attorney Questions
- Spinal cord stimulation (SCS) is a neuromodulation procedure in which an implanted pulse generator delivers electrical impulses through epidurally placed leads to the dorsal columns of the spinal cord, interrupting or modulating chronic pain signals before they reach the brain. SCS is used for conditions including CRPS, post-laminectomy syndrome, and refractory peripheral neuropathic pain. Unlike ablative procedures, SCS is reversible — the device can be turned off, reprogrammed, or explanted. In litigation, SCS arises when it has been performed and its necessity or cost is disputed, or when it is proposed as future care in personal injury damages analysis.
- Established SCS indications with clinical guideline and evidence support include: Complex Regional Pain Syndrome (CRPS) Type I and Type II; post-laminectomy syndrome (failed back surgery syndrome) with persistent radicular or axial pain; refractory peripheral neuropathic pain; painful diabetic neuropathy; and in some cases refractory angina and peripheral vascular disease. Medical necessity review addresses whether the specific diagnosis documented in the clinical record falls within recognized indications, whether the clinical course supports the indication, and whether the required evaluation and conservative treatment trial has been completed before proceeding to implantation.
- Yes. CRPS is one of the strongest evidence-supported indications for SCS. Randomized controlled trials have demonstrated that SCS produces superior pain relief compared to physical therapy alone in CRPS, and SCS is listed as a recommended therapy in published CRPS treatment guidelines including those from the Royal Dutch Society of Physical Therapy and others. In personal injury litigation, SCS for CRPS frequently arises as a future care item — the implant cost, battery replacement cycles, and programming costs constitute a significant component of long-term damages. The causal question is whether the CRPS diagnosis is supported by the clinical record and whether it is attributable to the subject accident or injury.
- Before permanent SCS implantation, the clinical record should document: an established diagnosis consistent with a recognized SCS indication; a documented course of conservative and conventional treatment that has failed to provide adequate relief; pre-implant psychological evaluation by a qualified mental health provider; a successful SCS trial stimulation with documented percentage improvement in pain (typically at least 50%) and functional status; and informed consent addressing the nature of the device, the trial and permanent implant procedures, risks, expected outcomes, and the requirement for ongoing maintenance. Absence of any of these elements — particularly the trial stimulation result and the psychological screening — is a recurring standard of care and medical necessity issue in SCS litigation.
- A successful SCS trial is generally defined as a reduction in pain intensity of at least 50%, assessed through validated pain outcome measures obtained both before and during the trial period. Some clinical protocols and payer criteria also require documented improvement in functional status or reduction in analgesic use as secondary measures of success. The trial period typically lasts seven to ten days. Contemporaneous documentation of baseline pain scores before the trial and follow-up pain scores during the trial period is critical — both to support the clinical decision to proceed to permanent implantation and as the evidentiary record in medical necessity review. Absence of documented pre-trial baselines or post-trial outcome measures is a recurring medical necessity and standard of care issue.
- Yes. Battery replacement is a predictable and documented component of long-term SCS management. Non-rechargeable implantable pulse generators typically require replacement every two to five years depending on stimulation parameters and usage. Rechargeable systems have longer projected battery life but still require eventual replacement. Future care projections for patients with SCS should account for: periodic battery replacement cycles at intervals consistent with the device type; the cost of each replacement procedure including surgery center and surgeon fees; lead revision procedures where clinically indicated by the prior course; and ongoing programming and device management visits. These are recurring, projectable costs with established market pricing and constitute a significant component of long-term damages in cases involving SCS.
- Device and procedural complications reviewed in SCS malpractice matters include: lead migration (displacement of the stimulation lead from the target position, resulting in loss of coverage or unwanted stimulation); lead fracture or hardware failure; epidural hematoma or seroma at the implant site; infection — ranging from superficial wound infection to deep hardware infection requiring explantation; spinal cord or nerve injury from lead placement or revision; inadequate trial result leading to permanent implantation that fails to replicate trial relief; and selection errors where implantation was performed in patients who did not meet appropriate selection criteria. The standard of care analysis addresses whether each complication resulted from a recognized risk of the procedure or from a technical deviation.
- Battery replacement cost projections require identification of the device type implanted (rechargeable vs. non-rechargeable), the manufacturer's projected battery life under typical usage conditions, the patient's age and life expectancy, and the current market cost of replacement procedures in the patient's geographic treatment area. Non-rechargeable IPG replacement costs include the device itself, the surgical facility fee, and the implanting physician fee. Defense review of a plaintiff's future care projection addresses whether the replacement frequency assumed in the projection is consistent with the device type and usage parameters, whether the projected costs reflect current market pricing, and whether the assumed duration of SCS need is supported by the clinical record.
- Key records include: complete treating pain management records from initial evaluation through the most recent encounter; the pre-implant psychological evaluation report; pre-trial pain outcome measures and the documented trial stimulation result; the trial and permanent implantation operative reports and device records (device model, lead placement, programming parameters); post-implant programming records and follow-up clinical notes documenting ongoing pain relief and functional status; imaging studies documenting lead position; records of any revision procedures or complications; billing records itemized by procedure and service; insurance authorization records; prior treating physician records predating the pain management relationship; and, where applicable, any device manufacturer documentation regarding the specific system implanted.
- Yes. Dr. Dardashti accepts SCS engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides. Review is available for the full scope of SCS-related issues — medical necessity, standard of care, causation of the underlying condition, and future medical care — or for a defined subset of those issues depending on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain an SCS Expert for Your Case
Dr. Dardashti accepts SCS engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.