Nationwide Pain & Injury Medical Expert Witness
Intrathecal Pump Therapy Expert Witness
Expert evaluation of intrathecal drug delivery systems — patient selection, device complications, catheter malfunction, granuloma formation, baclofen withdrawal, medical necessity, and future medical care projections in personal injury and medical malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Topic
- Intrathecal Drug Delivery Systems (IDDS)
- Also Known As
- Intrathecal Pump, Baclofen Pump, IT Pump
- Specialty
- Pain Management & Anesthesiology
- Evaluation Areas
- Causation, Device Complications, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Intrathecal Pump Therapy in Medical-Legal Review
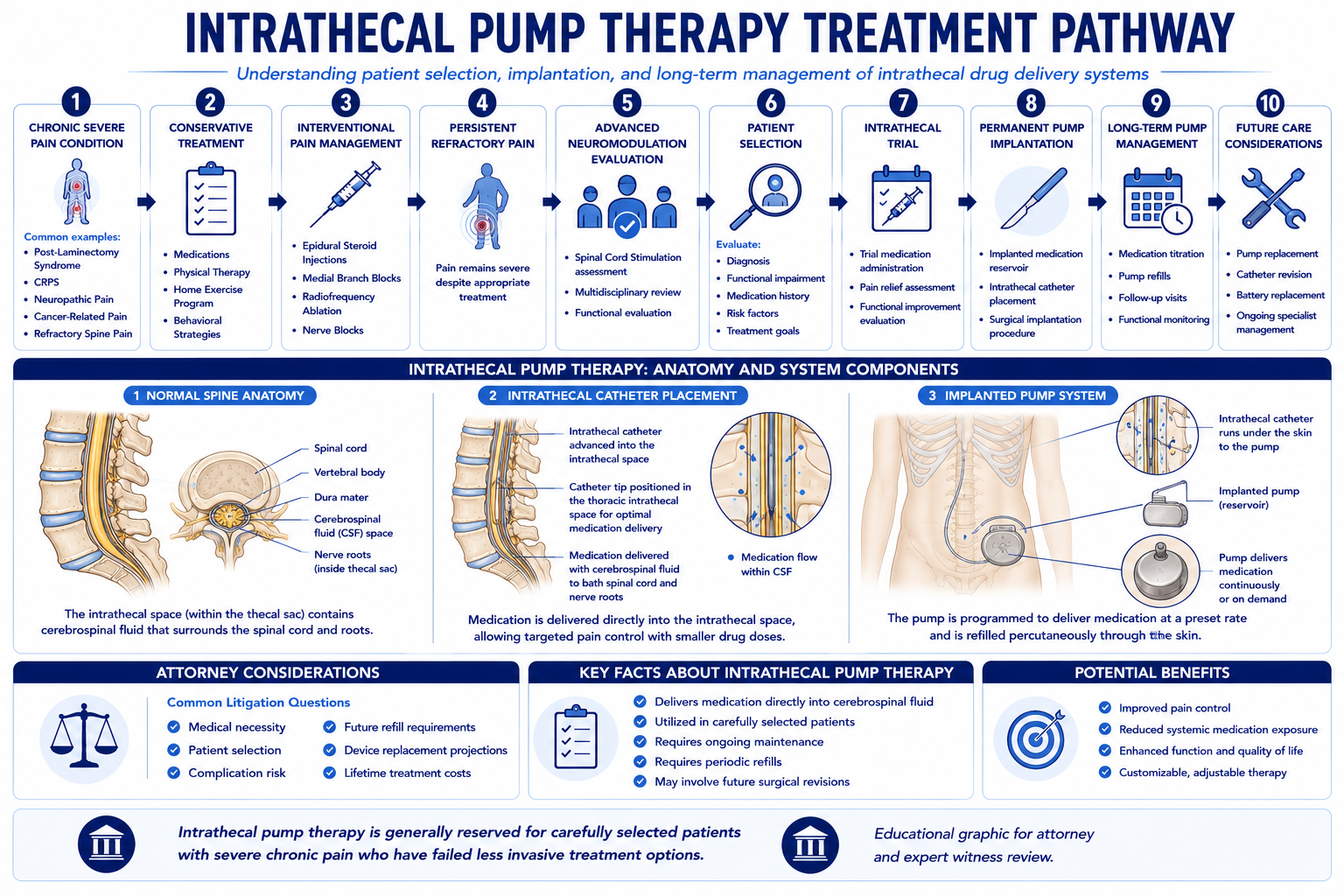
Intrathecal drug delivery systems — surgically implanted programmable pumps that deliver medication directly into the intrathecal space surrounding the spinal cord — represent one of the most advanced and cost-intensive interventions in pain management. IDDS bypasses the blood-brain barrier and the dose-limiting systemic effects of oral or intravenous medications, delivering effective drug concentrations at the spinal cord level at doses that may be three hundred times smaller than equivalent systemic doses. This pharmacological efficiency is both the clinical rationale for the therapy and the source of its most serious complication risks.
In litigation, intrathecal pump therapy arises across multiple case types. In personal injury matters, IDDS appears as a proposed future care item in cases involving severe chronic pain conditions — particularly refractory post-laminectomy syndrome and Complex Regional Pain Syndrome — where conventional management has been exhausted. In medical malpractice, IDDS cases involve device complications ranging from catheter malfunction and infection to granuloma formation with spinal cord compression and acute drug withdrawal with life-threatening consequences.
Expert review addresses the pain management dimensions of these cases — clinical appropriateness, patient selection, standard of care, complications, and future care projections. Opinions on neurosurgical implantation technique or device engineering are outside this scope. Contact Expert Medical Services LLC with a brief case summary to confirm scope and availability.
Conditions Commonly Treated with Intrathecal Drug Delivery
Intrathecal pump therapy is reserved for patients with severe, chronic pain or spasticity that has failed to respond adequately to systemic pharmacological management and to appropriate interventional pain procedures. The conditions most commonly giving rise to IDDS implantation in the litigation context reflect this advanced-refractory profile:
- › Post-laminectomy syndrome — Persistent spinal pain following spinal surgery is the most common non-cancer indication for IDDS in the United States. When prior surgery for disc herniation, stenosis, or deformity fails to relieve pain, and when subsequent pain management interventions — including epidural steroid injections, medial branch blocks, and spinal cord stimulation — are inadequate or contraindicated, IDDS becomes a therapeutic option. In personal injury litigation, the causal chain from the subject accident to spinal surgery to post-laminectomy syndrome to eventual IDDS implantation is a recurring damages pathway.
- › Refractory CRPS — Complex Regional Pain Syndrome refractory to physical therapy, pharmacological management, sympathetic nerve blocks, and spinal cord stimulation may be considered for intrathecal drug delivery, particularly when SCS has failed or is contraindicated due to prior spinal instrumentation or the presence of a cardiac pacemaker. IDDS in CRPS typically uses intrathecal opioids, ziconotide, or combination infusions targeting the neuropathic pain mechanisms underlying the syndrome.
- › Cauda equina syndrome sequelae — Cauda equina syndrome with permanent neurological injury can produce intractable neuropathic pain — perineal pain, bilateral lower extremity pain, and dysesthetic pain in denervated distributions — that is poorly responsive to systemic medications. IDDS may be considered for intractable neuropathic pain in this context when conservative interventional management has failed.
- › Spasticity from spinal cord injury or neurological disease — Intrathecal baclofen therapy is the most established IDDS application for spasticity management in patients with spinal cord injury, multiple sclerosis, cerebral palsy, and traumatic brain injury with severe spasticity. Baclofen delivered intrathecally achieves concentrations at spinal cord receptors that cannot be reached with oral dosing without dose-limiting sedation and cognitive effects.
- › Cancer pain — Intrathecal drug delivery for cancer pain has a distinct and stronger evidence base than the chronic non-cancer pain indications. Randomized controlled evidence supports IDDS as superior to systemic medical management for refractory cancer pain, and cancer pain IDDS typically involves high-concentration opioid infusions. Litigation involving cancer-related IDDS commonly addresses future care projections in catastrophic injury cases, device complications, and medication management errors.
Cancer Pain vs. Non-Cancer Pain Indications
The distinction between cancer and non-cancer pain as IDDS indications is clinically and medico-legally significant. The two populations have different evidence profiles, different selection thresholds, and different expectations about treatment duration and clinical trajectory.
For cancer pain, the Smith et al. randomized controlled trial — published in JAMA — demonstrated that IDDS produces clinically meaningful advantages over comprehensive systemic medical management in pain control and toxicity. The threshold for cancer pain IDDS implantation reflects the urgency and limited life expectancy of the cancer population: patients who have failed systemic opioid management may be considered for IDDS without the extended conservative treatment timeline required for non-cancer indications. Cancer pain IDDS typically involves high-dose opioid infusions and carries a distinct granuloma risk profile that informs surveillance protocols.
For non-cancer chronic pain, the evidence base is more limited and the selection criteria are more stringent. The Polyanalgesic Consensus Conference (PACC) guidelines — which establish the standard of care framework for IDDS in chronic non-cancer pain — require documented failure of multiple conservative treatment modalities before IDDS is considered appropriate. The clinical rationale for the higher threshold in non-cancer pain reflects both the more limited evidence base and the substantially longer treatment duration anticipated in a non-cancer population with normal or near-normal life expectancy.
In litigation, the cancer vs. non-cancer distinction is directly relevant to medical necessity review: what constitutes adequate pre-implant evaluation for a cancer pain patient differs materially from the requirements for a chronic non-cancer pain indication. Defense review of a non-cancer IDDS implant that was performed following a conservative treatment course inadequate for the non-cancer standard may identify standard of care issues that would not apply if the same implant were performed for refractory cancer pain.
Patient Selection Criteria
Appropriate patient selection for intrathecal drug delivery is a threshold element of the medical necessity and standard of care analysis. The selection process for non-cancer chronic pain indications involves a multidisciplinary evaluation addressing clinical, psychological, and practical dimensions of candidacy.
- › Diagnosis within a recognized indication — The patient's diagnosis must fall within an indication category for which clinical evidence supports intrathecal drug delivery. An IDDS implantation for a pain condition that does not meet any recognized indication is a medical necessity concern regardless of whether the patient reports benefit from the therapy.
- › Documented failure of prior treatments — The PACC guidelines require documented failure of adequate trials of pharmacological management, physical therapy, and appropriate interventional procedures before IDDS is considered for non-cancer chronic pain. Escalation to IDDS without a documented prior treatment course is a recognized medical necessity concern.
- › Psychological evaluation — Pre-implant psychological screening by a qualified mental health provider is a standard of care requirement for IDDS candidacy in non-cancer pain. The evaluation assesses untreated psychiatric comorbidities, active substance use disorder, cognitive capacity to manage the device, realistic expectations about treatment outcomes, and psychosocial factors that may affect IDDS response. Implantation without psychological screening is a departure from the standard and a recurring standard of care issue in IDDS litigation.
- › Medical clearance and contraindication review — Active systemic infection, coagulopathy, anatomical barriers to catheter placement, and allergy to the proposed intrathecal agent are contraindications to IDDS that must be assessed before implantation. Patients on anticoagulation require planned anticoagulation management consistent with neuraxial procedure guidelines.
- › Successful drug trial — A documented, successful intrathecal drug trial is both a standard of care requirement and a medical necessity prerequisite. The trial confirms that intrathecal delivery of the proposed agent produces clinically meaningful pain relief with acceptable tolerability before the patient undergoes a surgical implantation procedure.
The Trialing Process
The intrathecal drug trial is the mandatory pre-implant assessment that evaluates the patient's response to intrathecal drug delivery before a permanent pump is implanted. Unlike the spinal cord stimulation trial — which typically lasts seven to ten days with temporary external hardware — the IDDS trial may be performed as a single-dose intrathecal bolus injection through a standard lumbar puncture, or as a multi-day continuous infusion through a temporarily implanted intrathecal catheter connected to an external pump.
The bolus trial method provides a rapid assessment of medication response but does not replicate the continuous delivery kinetics of a permanent pump. The continuous infusion trial — performed in an inpatient or monitored outpatient setting — more closely approximates the pharmacological environment of the implanted system but requires a short-term surgical procedure to place the temporary catheter. The choice of trial method is a clinical judgment based on the proposed drug, the patient's clinical circumstances, and the treating physician's experience.
Regardless of method, the trial documentation must capture: baseline pain scores using a validated instrument (VAS or NRS) before the trial; post-trial pain scores using the same instrument; the percentage improvement in pain; functional observations during the trial period; any side effects experienced; and the treating physician's clinical assessment of trial success or failure. A meaningful reduction in pain intensity — typically defined as at least 50% improvement — with tolerable side effects constitutes a successful trial supporting permanent implantation.
In litigation, the trial documentation is the central evidentiary record for medical necessity review of permanent implantation. Implantation without a documented trial, or proceeding to permanent implantation after a documented trial failure, is a standard of care deviation. The absence of contemporaneous pre-trial and post-trial pain scores — even when the physician reports the trial was successful — creates an evidentiary gap that may not be resolved by retrospective characterization.
Surgical Implantation Procedure
Permanent IDDS implantation is a two-component surgical procedure: intrathecal catheter placement and pump pocket creation. The catheter is introduced into the intrathecal space at the lumbar level under fluoroscopic guidance and advanced to the target level determined by the pain distribution — lower thoracic levels for lower extremity and lumbar pain, and upper thoracic or cervical levels for thoracic or upper extremity pain conditions. The catheter is then tunneled subcutaneously to the pump pocket — typically created in the abdominal subcutaneous tissue or the flank — where it is connected to the programmable pump.
Fluoroscopic guidance is required for catheter placement to confirm intrathecal entry, catheter position, and target level. The final catheter tip position is documented radiographically as part of the operative record and is relevant to both the appropriateness of the delivery site and the analysis of catheter-tip complications — particularly granuloma formation.
The implantation procedure is substantially more invasive than the trial procedure and carries a distinct and more significant risk profile — including the risks of infection at the incision and pocket sites, catheter-related bleeding, post-dural puncture headache, cerebrospinal fluid leak, catheter malposition, and the anesthetic risks of the surgical procedure itself. The informed consent process should address these risks specifically, and their documentation in the preoperative record is relevant to standard of care review in complication cases.
Medication Selection and Pharmacology
The Polyanalgesic Consensus Conference guidelines provide a tiered algorithm for intrathecal drug selection in chronic non-cancer pain based on the level of evidence supporting each agent. The choice of medication — or combination of medications — is one of the most consequential clinical decisions in IDDS management, with direct implications for efficacy, side effect profile, and the risk of catastrophic complications, particularly granuloma formation.
- › Morphine — The most extensively studied and FDA-approved intrathecal analgesic for chronic pain. Morphine is a first-line PACC recommendation and the most commonly used agent in chronic non-cancer pain IDDS. High-concentration intrathecal morphine carries the highest granuloma risk among the commonly used agents and requires granuloma surveillance protocols.
- › Ziconotide — An N-type calcium channel blocker derived from cone snail venom and the only FDA-approved non-opioid intrathecal analgesic. Ziconotide carries no granuloma risk but has a narrow therapeutic window and significant neurological side effects — including cognitive impairment, hallucinations, dizziness, and nystagmus — that require careful dose titration and clinical monitoring. Ziconotide is a PACC first-line recommendation alongside morphine for nociceptive and neuropathic pain.
- › Hydromorphone — A semisynthetic opioid used as an alternative to morphine with a somewhat lower granuloma risk profile. Hydromorphone is a second-tier PACC recommendation for chronic non-cancer pain when first-line agents are inadequate or not tolerated.
- › Baclofen — The primary agent for intrathecal baclofen therapy (ITB) for spasticity. Baclofen is a GABA-B receptor agonist and does not carry opioid-related granuloma risk, but intrathecal baclofen withdrawal — from catheter failure, empty reservoir, or pump malfunction — is a potentially life-threatening emergency requiring prompt recognition and systemic baclofen rescue.
- › Admixtures and combination therapy — Intrathecal combinations of opioids with adjuvants such as bupivacaine or clonidine are used in clinical practice when single-agent therapy is inadequate. The PACC guidelines address evidence and risk profiles for these combinations, and polypharmacy decisions in IDDS management may be relevant to standard of care review when adverse outcomes are associated with combination infusions.
The drug selection decision, the concentration prescribed, and the dose titration pathway are all subject to standard of care review when complications — particularly granuloma — are alleged to have resulted from inappropriate drug or concentration choices.
Pump Refills and Ongoing Maintenance
Intrathecal pump therapy requires scheduled, lifelong clinical maintenance centered on drug refill procedures and device interrogation. The pump reservoir must be refilled at intervals determined by the reservoir volume, the drug concentration, and the programmed infusion rate — typically every four to twelve weeks in clinical practice, though high-dose regimens may require more frequent refills.
Each refill procedure involves percutaneous needle access to the pump reservoir using a non-coring needle and template-guided technique, withdrawal of the residual drug volume, refilling with the prescribed solution, and electronic interrogation of pump function and programming. The refill visit also provides an opportunity for clinical assessment of pain control, side effects, and any symptoms suggesting device malfunction or catheter complications.
- › Refill errors and medication mix-ups — Medication errors during the refill procedure — including filling the pump with the wrong concentration, the wrong drug, or injecting medication into the subcutaneous tissue rather than the reservoir — are a recognized source of serious adverse events. Errors that result in drug overdose or underdose may present as sudden neurological deterioration or acute withdrawal and constitute both a medication safety and standard of care concern.
- › Reservoir depletion and withdrawal risk — Failure to schedule timely refills — or failure to communicate to the patient the importance of keeping scheduled refill appointments — can result in drug depletion, cessation of drug delivery, and acute withdrawal syndrome. For baclofen-dependent patients, reservoir depletion is a medical emergency. Documentation of the refill schedule, patient education, and follow-up protocols is relevant to standard of care review in withdrawal cases.
- › Drug stability and compounding — Intrathecal drug solutions — particularly compounded admixtures — must meet stability requirements appropriate for the reservoir residence time between refills. Stability failures can result in degraded medication delivery and loss of pain control. In cases where compounded intrathecal solutions are used, the compounding pharmacy's compliance with applicable sterility and stability standards is a relevant review area.
In future medical care projections, refill visits represent the highest-frequency and most reliably recurring cost component of long-term IDDS management. The projected number of refill visits per year, multiplied by the cost per visit including physician fee, facility fee, and drug cost, produces a substantial recurring annual expense that must be itemized and priced to the patient's treating market.
Device Replacement and Battery Life
Intrathecal pumps contain internal batteries with finite life expectancy. Battery end-of-life is reached when the pump can no longer maintain accurate drug delivery — at which point the pump must be surgically replaced. Pump replacement is a separate surgical procedure in which the pocket is reopened, the depleted pump is disconnected from the intrathecal catheter, and a new pump is connected and implanted. The catheter is retained and reused if it is intact and properly positioned.
Battery life varies by device manufacturer, pump model, and usage parameters — particularly the programmed infusion rate. Current generation programmable IDDS pumps have projected battery life of approximately five to seven years under typical clinical usage conditions, though high-flow rate programs associated with aggressive pain management protocols may result in shorter battery life. The treating physician and refill team monitor battery depletion through electronic interrogation at each refill visit and schedule elective pump replacement before the battery reaches the end of its operational capacity.
In future care projections, the number of pump replacements over the patient's life expectancy is calculated based on the expected device life of the implanted pump model. Each replacement surgery involves facility fees, surgeon fees, and the cost of the replacement pump device itself — which may exceed ten thousand dollars per procedure. Over the life expectancy of a young patient, pump replacement surgeries may constitute the single largest component of the total IDDS cost projection, and defense review addresses whether the projected replacement interval is consistent with the device type and clinical usage parameters rather than a generically shortened interval.
Infection Complications
Infection is one of the most serious and clinically consequential complications of intrathecal drug delivery systems. IDDS infections range in severity from superficial wound infections that may resolve with antibiotics to deep pocket infections and meningitis that require complete hardware explantation. The presence of a foreign body in proximity to the central neuraxis makes the clinical consequences of infection disproportionately severe relative to an equivalent soft tissue infection in another anatomical location.
- › Pocket infection — Infection of the subcutaneous pump pocket — most commonly presenting as wound erythema, swelling, warmth, and purulent discharge — typically requires explantation of the pump to allow definitive treatment of the infected pocket. Salvage of an infected pump with antibiotics alone is generally not successful and attempts to do so may allow the infection to spread.
- › Meningitis — Bacterial meningitis following IDDS placement — resulting from direct contamination of the intrathecal catheter or from hematogenous seeding — is a life-threatening emergency requiring prompt diagnosis, appropriate antibiotic therapy, and management in an appropriate care setting. Meningitis associated with IDDS may necessitate complete system explantation. Delay in recognizing intrathecal infection and initiating appropriate treatment is a recurring standard of care issue in serious infection cases.
- › Standard of care considerations — Infection prevention measures include perioperative prophylactic antibiotics, sterile surgical technique during implantation and refill procedures, appropriate patient selection (excluding patients with active systemic infection), and wound care instructions and follow-up. Standard of care review in infection cases addresses whether each of these measures was documented and appropriately performed, and whether early infection signs were identified and acted upon at the appropriate clinical stage.
- › Explantation consequences — Explantation of an infected IDDS represents a significant clinical harm in addition to the infection itself: the patient is deprived of the pain control or spasticity management the device was providing, must undergo a second surgical procedure, and — if reimplantation is later pursued — must repeat the full trial-to-implantation sequence. The cumulative harm of the infection and explantation is a component of damages in IDDS infection malpractice claims.
Catheter Complications
The intrathecal catheter is the most mechanically vulnerable component of the IDDS system. Catheter complications — including migration, kinking, disconnection, occlusion, and fracture — are a recognized and relatively common source of therapy failure and may have serious clinical consequences depending on the medication being delivered and the speed of clinical recognition.
- › Catheter migration — Displacement of the catheter tip from the intended spinal level to a more caudal or cephalad position alters drug distribution and may result in either inadequate pain control (if the catheter migrates away from the target) or unintended effects (if the catheter migrates toward higher spinal cord levels). Migration may be identified on fluoroscopy or CT myelography when pump function checks or symptom changes prompt investigation.
- › Catheter disconnection — Disconnection of the catheter from the pump at the connector junction results in complete cessation of drug delivery, with the clinical presentation determined by the drug being delivered. Opioid catheter disconnection produces acute opioid withdrawal — with autonomic symptoms, pain crisis, and potentially serious cardiovascular effects — while baclofen disconnection produces acute baclofen withdrawal, a potentially life-threatening syndrome.
- › Catheter occlusion — Partial or complete occlusion of the catheter lumen impairs drug delivery. Granuloma formation at the catheter tip is a specific and serious form of catheter occlusion with distinct pathophysiology and clinical consequences, addressed separately below.
- › Imaging and diagnostic limitations — Catheter complications can be difficult to identify on standard imaging. Plain fluoroscopy shows catheter position but not patency. CT myelography — which involves injection of contrast through the pump sideport to evaluate catheter integrity and flow — is the most reliable method for identifying catheter disconnection, occlusion, and migration, but even this technique has limitations in complex cases with prior spinal instrumentation. The appropriate diagnostic workup for suspected catheter failure is a standard of care consideration in cases where delayed diagnosis of a catheter complication resulted in prolonged drug delivery failure.
Intrathecal Granuloma Formation
Intrathecal granuloma — also termed inflammatory mass or catheter-tip granuloma — is a benign but potentially catastrophic complication of IDDS in which an inflammatory mass forms at the tip of the intrathecal catheter in response to concentrated drug delivery, most commonly associated with high-concentration morphine infusions. The pathophysiology involves inflammatory and granulomatous reaction to the sustained presence of opioid drug at the catheter tip in the intrathecal space.
Granulomas typically develop gradually over weeks to months, initially causing progressive loss of analgesic efficacy — which may prompt dose escalation that paradoxically accelerates granuloma growth — and eventually producing neurological signs and symptoms from mass effect on the spinal cord or cauda equina. The classical clinical presentation includes progressive pain worsening, dose escalation without proportional pain relief, and the subsequent development of new sensory or motor deficits in the distribution of the compressed neural structures.
- › Risk factors — Recognized granuloma risk factors include high intrathecal drug concentration (particularly morphine), high daily dose, catheter tip placement at thoracic levels, and prolonged therapy duration. PACC guidelines provide drug concentration limits designed to minimize granuloma risk, and prescribing above these limits without documented clinical justification is a potential standard of care concern.
- › Surveillance and monitoring — Current IDDS management guidelines recommend clinical surveillance for granuloma in patients on intrathecal opioids — particularly monitoring for unexplained loss of analgesic efficacy, progressive dose escalation, or new neurological symptoms. MRI with gadolinium is the preferred imaging modality when granuloma is suspected. Failure to maintain appropriate surveillance and to investigate unexplained analgesic failure promptly are standard of care concerns in cases where delayed diagnosis resulted in cord compression and permanent neurological injury.
- › Management and litigation implications — Management of confirmed granuloma depends on clinical urgency. Emergent surgical decompression is required when neurological deficits are progressing rapidly. In less acute presentations, drug cessation with close clinical monitoring allows gradual granuloma resolution in many cases. The adequacy of the clinical response — particularly the timing of imaging and surgical intervention when neurological deficits were present — is the central issue in granuloma malpractice claims. Permanent neurological injury from delayed decompression of a symptomatic granuloma is a severe and irreversible harm with significant damages implications.
Medical Necessity Analysis
Medical necessity for intrathecal drug delivery in non-cancer chronic pain is evaluated against the PACC guidelines and the clinical record. A medically supported IDDS implant requires documentation of each of the threshold elements of the selection criteria: a diagnosis within a recognized indication, documented failure of prior treatments, completed psychological evaluation, clearance from contraindications, a successful and documented drug trial, and a treating physician's clinical rationale connecting all of these elements to the implantation decision.
Defense review of IDDS medical necessity addresses whether the pre-implant evaluation documented in the clinical record meets these requirements. Common grounds for medical necessity challenges include: inadequate documentation of the prior treatment course and its failure; absence of psychological screening; implantation after a drug trial that was not formally documented or did not meet the success threshold; and implantation for a pain condition that does not fall within a recognized IDDS indication.
In personal injury matters, medical necessity analysis operates at two levels. The first is whether the underlying condition — for example, post-laminectomy syndrome or refractory CRPS — is causally related to the subject accident. The second is whether, given the documented clinical course of that condition, intrathecal pump implantation was medically necessary and appropriate in the specific patient. These analyses are distinct but interdependent: a condition that is causally related to the accident may still not meet the clinical threshold for IDDS, and the necessity analysis must be grounded in the documented treatment course rather than in assumptions about what a plaintiff's condition might eventually require.
Plaintiff review of IDDS medical necessity addresses whether the treating physician's records adequately document the clinical basis for implantation and whether the PACC selection criteria are satisfied — both to support the claim that the implant was appropriate and to respond to anticipated defense challenges on necessity grounds. For the broader medical necessity framework governing implanted neuromodulation devices — including selection criteria, prior conservative care documentation, and trial requirements — see the article on how pain management experts evaluate medical necessity for spinal cord stimulators.
Standard of Care Considerations
The standard of care for intrathecal drug delivery system management reflects the practice of a reasonably competent board-certified pain management physician operating within applicable clinical guidelines — including the Polyanalgesic Consensus Conference guidelines and published society recommendations for IDDS implantation, programming, and long-term management. Core standard of care elements span the full IDDS lifecycle from patient selection through ongoing maintenance.
- › Appropriate selection and pre-implant evaluation — Completion of the full pre-implant evaluation sequence — psychological screening, documentation of prior treatment failure, drug trial, and medical clearance — before proceeding to permanent implantation is a threshold standard of care requirement. Bypassing any component of this sequence is a recognized deviation.
- › PACC-compliant drug selection and concentration — Selection of drug agents and concentrations consistent with the PACC algorithm, including adherence to published concentration limits associated with granuloma risk, is a standard of care consideration in drug-related complication cases.
- › Safe refill procedures — Refill procedures must be performed with proper identification of the pump reservoir port, correct needle technique, verification of drug identity and concentration, and pump interrogation to confirm delivery. Failure to identify the correct port, use of the wrong drug or concentration, or omission of pump interrogation are procedural deviations with the potential for serious patient harm.
- › Granuloma surveillance — The standard of care for patients on intrathecal opioids — particularly high-concentration morphine — includes clinical monitoring for signs suggesting granuloma: progressive analgesic failure, unexplained dose escalation, and new neurological symptoms. Prompt imaging evaluation when these features are present, and urgent surgical consultation when neurological deficits develop, are standard of care requirements in granuloma cases.
- › Withdrawal prevention and emergency planning — Patients receiving intrathecal opioids or intrathecal baclofen must be educated about withdrawal risk, signs and symptoms of device failure, and the importance of scheduled refill appointments. The treating physician should have an emergency management protocol for device failure and should ensure that the patient and relevant caregivers understand the withdrawal emergency and how to respond.
Future Medical Care Considerations
Intrathecal drug delivery generates a complex, lifelong future care cost structure that must be carefully analyzed and itemized in personal injury damages assessment. IDDS future care projections are among the most involved in pain management litigation because they combine recurring high-frequency components — refill visits — with periodic surgical events — device replacement and possible catheter revision — and unpredictable but statistically expected complication management costs.
A defensible future medical care projection for an IDDS patient must ground each cost component in the patient's specific clinical circumstances — the drug and concentration used, the pump model implanted, the patient's age and life expectancy, the treating physician's documented management plan, and current market pricing for each component in the patient's geographic area. Generic projections that do not account for device-specific battery life, actual refill frequency, or geographic cost variation are vulnerable to challenge on both clinical and economic grounds.
Defense review of plaintiff IDDS future care opinions focuses on whether the projected cost components are individually supported, whether the assumed timelines are consistent with the implanted device specifications, whether the complication rates assumed are grounded in published data rather than worst-case assumptions, and whether any alternative management strategies — such as dose reduction, drug change to reduce granuloma risk, or transition to a less expensive modality — were inappropriately excluded from the analysis.
Cost of Ongoing IDDS Treatment
The aggregate cost of long-term intrathecal drug delivery management is substantial and can constitute a dominant component of future damages in catastrophic injury cases involving young patients. Key cost components include:
- › Drug trial procedure — The initial drug trial — whether a single-shot bolus or a multi-day catheter infusion — involves physician fees, facility fees, anesthesia where applicable, and monitoring costs. This is a one-time upfront cost in the treatment pathway.
- › Initial implantation surgery — The permanent pump implant involves the device cost (ranging from fifteen thousand to thirty thousand dollars or more depending on model and manufacturer), the surgical facility fee, the implanting physician fee, and anesthesia. This is typically the largest single-episode cost in the IDDS cost structure.
- › Drug refills — Each refill visit involves a physician fee, a facility or office fee, the cost of the compounded or commercially prepared drug, and any associated laboratory monitoring. At six to thirteen refill visits per year, the aggregate annual refill cost becomes a major recurring expense over the patient's lifetime.
- › Pump replacement surgeries — Each device replacement involves the same cost categories as the initial implant minus the catheter placement component, occurring at intervals of approximately five to seven years. Over a thirty- to forty-year life expectancy, this can represent four to eight replacement procedures at substantial per-procedure cost.
- › Catheter revision procedures — Published IDDS complication literature documents catheter revision rates that justify including a projected revision rate — typically expressed as a number of revisions over the patient's lifetime — based on published data rather than assuming zero catheter complications.
- › Granuloma surveillance imaging — Patients on intrathecal opioids who are at elevated granuloma risk may require periodic MRI surveillance, adding an imaging cost component to the ongoing management plan where clinically indicated by the drug, concentration, and clinical course.
Causation Analysis
Causation analysis in intrathecal pump cases operates on multiple levels depending on the case type. In personal injury matters where IDDS is proposed as future care, causation analysis addresses the causal chain from the subject accident to the condition ultimately requiring pump implantation — a multi-step analysis that must connect each clinical development in the chain to the initiating event.
The most common causal pathway in personal injury IDDS cases involves: (1) traumatic spinal injury from the subject accident; (2) spinal surgery indicated by that injury; (3) development of refractory post-laminectomy syndrome following surgery; (4) failure of conservative and interventional pain management for the post-laminectomy pain; (5) failure or contraindication of spinal cord stimulation; and (6) IDDS as the appropriate next management step. Causation review addresses whether each step in this chain is clinically documented and supported, and whether each step is causally linked to the step before it and ultimately to the subject accident.
Pre-existing conditions are frequently relevant in IDDS causation analysis. A patient with a prior history of back pain, prior spinal surgery, or a pre-existing diagnosis potentially relevant to the current pain condition requires specific causation analysis addressing whether the subject accident caused, materially aggravated, or was unrelated to the clinical picture. Aggravation causation — the subject event materially accelerated or worsened a pre-existing vulnerability — is a distinct but recognized theory that can support IDDS damages attribution even where the patient's underlying spine pathology predates the accident.
In malpractice matters where a device complication produced permanent harm, causation analysis addresses whether the physician's actions or omissions were the proximate cause of the specific harm alleged — distinct from whether IDDS in general was appropriate for the patient. These are separate analyses and require careful structuring when the malpractice claim involves both a selection error and a management complication in the same clinical course.
Independent Medical Evaluations
Independent medical evaluation of an IDDS patient requires examination that is adapted to the specific clinical circumstances of a patient with an implanted device. Physical examination includes assessment of the pump site for signs of infection, erosion, or migration of the implanted hardware; evaluation of the catheter tunneling pathway; and neurological examination of the extremities relevant to the condition being treated and to any alleged complications.
In personal injury matters where IDDS is proposed as future care rather than existing treatment, the IME focuses on the current clinical status of the underlying condition — assessing whether the clinical findings, functional status, and treatment course support the proposition that IDDS will be required in the future. This requires review of all prior treatment records as well as physical examination findings documented contemporaneously at the time of the evaluation. For the full pain management examination methodology — range-of-motion testing, motor and sensory assessment, validated functional instruments, and symptom validity evaluation — see the article on how pain management experts objectively evaluate pain.
In malpractice matters involving alleged device complications, the IME addresses the current neurological and pain status in relation to the claimed harm, whether current findings are consistent with the alleged complication mechanism, and what ongoing care the patient requires as a result of the complication. Cases requiring physical assessment should be structured as an independent medical evaluation; records-based engagements that do not require examination are also available and are structured based on the questions retaining counsel needs addressed.
Common Litigation Scenarios
Intrathecal pump cases present a defined set of recurring litigation patterns across personal injury and medical malpractice contexts.
- › Personal injury with IDDS as proposed future care — A plaintiff with refractory post-traumatic spinal pain or CRPS whose treating pain management physician recommends IDDS implantation as the next treatment step. The plaintiff's life care plan or future care expert projects IDDS costs over the plaintiff's life expectancy. Defense review addresses whether the clinical course supports the IDDS recommendation, whether the prior treatment pathway is adequately documented, and whether the projected IDDS cost components are individually supported and appropriately priced. For California, Texas, and Nevada-based matters, see the California, Texas, and Nevada expert witness pages.
- › Malpractice — granuloma with neurological injury — A patient on intrathecal morphine develops progressive neurological deficits from a catheter-tip granuloma. The claim addresses whether the physician maintained adequate granuloma surveillance, whether early symptoms prompted appropriate investigation, and whether surgical decompression was initiated at a clinically appropriate time. Cases involving permanent cord injury or paraplegia carry significant damages.
- › Malpractice — acute baclofen withdrawal — A patient with intrathecal baclofen for spasticity develops acute withdrawal syndrome following catheter disconnection or reservoir depletion, presenting with hyperpyrexia, extreme muscle rigidity, rhabdomyolysis, and — in severe cases — multi-organ failure and death. The claim addresses whether the catheter failure was identifiable at an earlier clinical stage, whether the patient was educated about withdrawal risk and device failure signs, whether the clinical team recognized the withdrawal syndrome when it presented, and whether appropriate emergency treatment was initiated promptly.
- › Malpractice — refill error resulting in drug overdose or underdose — A refill procedure error — wrong drug, wrong concentration, or injection into subcutaneous tissue rather than the pump reservoir — produces acute overdose or underdose. Overdose cases may present as respiratory depression, altered consciousness, or death; underdose or withdrawal cases present as pain crisis or, for baclofen, as withdrawal syndrome. The claim addresses the procedural conduct of the refill and the safeguards that were or were not in place.
Expert Witness Review Process
Intrathecal pump cases require review of a defined record set to support a complete medical-legal opinion. The specific records relevant to the engagement depend on the scope defined by retaining counsel. Key records include:
- › Complete treating pain management records — Initial evaluation, follow-up notes, procedure records, and drug programming logs from the beginning of the pain management relationship through the most recent visit, including all refill visit documentation
- › Drug trial records — Pre-trial pain scores, trial procedure report, drug and dose administered, post-trial pain scores, and the treating physician's documented assessment of trial success or failure
- › Pre-implant psychological evaluation — Screening report addressing psychiatric diagnoses, substance use history, psychosocial factors, cognitive capacity, realistic expectations, and the evaluator's recommendation regarding IDDS candidacy
- › Implantation operative report and device records — Implant procedure report, catheter tip placement level documented fluoroscopically, pump model and serial number, initial programming parameters, and device specifications
- › Pump programming and refill records — Electronic interrogation records documenting drug concentrations, flow rates, programmed doses, reservoir volumes at each refill, and any programming changes with rationale
- › Imaging studies — Pre-implant spinal imaging; post-implant fluoroscopic catheter position records; MRI studies where granuloma or cord compression is at issue; CT myelography studies where catheter patency or migration is at issue
- › Prior treating records — Records predating the pain management relationship to establish the pre-injury baseline, document the prior treatment course, and assess the presence or absence of conditions relevant to causation or patient selection
- › Complication records — Hospital records, emergency department records, and specialist records documenting any IDDS complications — infection, withdrawal, overdose, granuloma, catheter failure — including treatment rendered and outcome
- › Billing and authorization records — Itemized billing and pre-authorization records where a medical necessity or coverage dispute is at issue
- › Deposition testimony — Testimony of the treating pain management physician, the implanting physician where applicable, the claimant, and any other experts addressing the medical issues at issue in the case
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. Engagements can be structured to address medical necessity, standard of care, causation, future medical care, or a combination of these questions within a single retention. For California matters see the California Pain Management Expert Witness page; for Texas matters see the Texas Pain Management Expert Witness page; for Nevada matters see the Nevada Pain Management Expert Witness page.
Related Services & Expertise
CRPS Expert Witness
CRPS refractory to conventional management is a recognized IDDS indication — diagnosis, causation, Budapest Criteria, and future care.
Spinal Cord Stimulation
SCS is typically evaluated before IDDS for pain indications — necessity, trial, device complications, and future care.
Future Medical Care Review
Projecting IDDS refill, monitoring, replacement, granuloma surveillance, and complication costs over the patient's life expectancy.
Causation Analysis
Linking the underlying condition requiring intrathecal pump therapy to the subject accident or injury.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California IDDS matters.
Texas Pain Management Expert Witness
Intrathecal pump therapy expert review for Texas personal injury and malpractice matters.
Nevada Pain Management Expert Witness
Intrathecal pump expert review for Nevada personal injury litigation.
Independent Medical Evaluation
Structured examination for IDDS patients where physical assessment is required alongside records review.
Arizona Pain Management Expert Witness
Intrathecal pump therapy expert review for Arizona personal injury litigation.
Florida Pain Management Expert Witness
Intrathecal pump therapy expert review for Florida personal injury and medical malpractice litigation.
Medical Necessity Review
Medical necessity review for intrathecal pump implantation — candidate selection, trial assessment, and device justification.
Standard of Care Analysis
Standard of care analysis for intrathecal drug delivery — trial protocol, dose management, and complication review.
FAQ
Intrathecal Pump Therapy — Common Attorney Questions
- An intrathecal drug delivery system (IDDS) is a surgically implanted pump that delivers medication directly into the intrathecal space — the fluid-filled space surrounding the spinal cord — at doses far smaller than those required for equivalent systemic effect. In litigation, IDDS cases arise in personal injury matters where pump implantation is proposed as future care, and in medical malpractice matters involving device complications or medication errors. The high cost of the device, the complexity of ongoing maintenance, and the severity of potential complications — particularly drug withdrawal and granuloma formation — make IDDS a substantial source of both damages analysis and standard of care disputes.
- Intrathecal pump therapy is indicated for chronic pain or spasticity that has proven refractory to systemic pharmacological management and to less invasive interventional pain procedures. In the personal injury litigation context, the most common conditions giving rise to IDDS implantation are refractory post-laminectomy syndrome — persistent spinal pain following failed back surgery — refractory Complex Regional Pain Syndrome that has failed spinal cord stimulation or where SCS is contraindicated, cauda equina syndrome with intractable neuropathic pain, and serious spinal cord injury producing intractable pain or spasticity requiring intrathecal baclofen. In cancer-related litigation and life care planning, intractable cancer pain inadequately controlled by systemic opioids is a recognized indication with a distinct evidence profile from chronic non-cancer pain applications.
- Cancer pain and non-cancer pain represent distinct indication profiles for intrathecal pump therapy, with different evidence bases, patient selection criteria, and litigation implications. For cancer pain, randomized controlled trial evidence — including the landmark Smith et al. study published in JAMA — demonstrates that IDDS produces superior pain control and reduced medication toxicity compared to comprehensive medical management alone, and IDDS is an established evidence-supported therapy in refractory cancer pain. For non-cancer chronic pain, the evidence base is less robust and the indication criteria are more stringent: the patient must have failed an adequate course of conservative and conventional interventional treatment, and psychological screening must be completed before implantation. In litigation, the distinction is material to both the medical necessity analysis and the causation inquiry — the threshold for IDDS in cancer pain is lower than in chronic non-cancer pain, and the expected clinical course differs substantially between the two populations.
- Before IDDS implantation for non-cancer pain, the clinical record should document: a diagnosis consistent with a recognized indication for intrathecal drug delivery; failure of an adequate trial of conservative treatment including pharmacological management, physical therapy, and appropriate interventional pain procedures; failure or contraindication of less invasive neuromodulation options such as spinal cord stimulation; a comprehensive psychological evaluation by a qualified mental health provider clearing the patient for implantable device therapy; a successful intrathecal drug trial demonstrating adequate pain relief with the proposed agent; and medical clearance confirming the patient is a safe surgical candidate. Absence of documented psychological screening, failure to complete a drug trial, or implantation without establishing refractoriness to prior treatments are recurring medical necessity and standard of care issues in IDDS litigation.
- The intrathecal drug trial is a pre-implantation test in which medication is administered directly into the intrathecal space — typically through a lumbar puncture or temporary intrathecal catheter — to evaluate whether intrathecal drug delivery produces adequate pain relief with acceptable side effects before a permanent pump is implanted. A successful trial is generally defined as a clinically meaningful reduction in pain intensity with tolerable side effects. The trial may be performed as a single-shot bolus injection or through a continuous infusion via a temporary catheter. Documentation of the trial — including the drug and dose administered, pre-trial and post-trial pain scores, the patient's subjective experience of the therapy, and any side effects observed — is the pivotal clinical record supporting permanent implantation and a central focus of medical necessity review. Permanent implantation without a documented, successful drug trial is a standard of care concern.
- Device-related and pharmacological complications reviewed in IDDS litigation include catheter malfunction (kinking, migration, disconnection, or tip occlusion), pump failure or programming error, intrathecal granuloma formation at the catheter tip, surgical site infection, meningitis, pocket infection requiring explantation, drug overdose from programming errors or pump refill errors, drug underdose or withdrawal from catheter disruption or empty reservoir, and in baclofen therapy specifically — acute intrathecal baclofen withdrawal, a potentially life-threatening syndrome characterized by hyperpyrexia, muscle rigidity, rhabdomyolysis, and multi-organ failure. Each complication type implicates a distinct standard of care analysis: whether the complication was a recognized risk managed appropriately, or whether it resulted from a clinical or technical deviation.
- An intrathecal granuloma — also called an inflammatory mass or catheter-tip granuloma — is a benign but potentially serious inflammatory mass that forms at the tip of the intrathecal catheter in response to concentrated medication delivery, most commonly with high-concentration opioid infusions. Granulomas can grow to compress the spinal cord or cauda equina, producing progressive neurological deficits including weakness, sensory loss, and bowel and bladder dysfunction. In litigation, granuloma cases raise questions of whether the prescribing physician was aware of the risk, whether appropriate surveillance imaging was obtained at clinically appropriate intervals, whether early neurological symptoms were recognized and acted upon promptly, and whether dose escalation that increased granuloma risk was clinically justified. Granuloma formation with cord compression and resulting permanent neurological injury is one of the most serious IDDS complications and carries significant damages implications.
- Medical necessity for IDDS is evaluated against the clinical record and applicable treatment guidelines. A supported indication requires documentation that the patient has a diagnosis within a recognized indication category; that an adequate course of conservative and interventional treatment has been completed and has failed to provide adequate relief; that less invasive implantable options — particularly spinal cord stimulation for pain indications — have been considered, failed, or are contraindicated; that psychological screening has been completed and clearance obtained; that the intrathecal drug trial was performed and produced a documented, meaningful response; and that the treating physician's clinical rationale clearly connects the patient's condition and treatment course to the proposed device. Defense review of IDDS medical necessity focuses on whether each of these threshold elements is documented in the clinical record and whether the timeline of treatment escalation is consistent with the progression from conservative management to implantable device therapy.
- Future medical care projections for IDDS patients are among the most complex in personal injury damages analysis because they involve multiple recurring cost components over the patient's life expectancy. A comprehensive IDDS future care projection includes: the cost of the drug trial procedure; pump implantation surgery including facility, device, and physician fees; drug refills at intervals determined by reservoir volume and pump flow rate — typically every four to twelve weeks depending on the drug concentration and dose; clinic visits for each refill and for ongoing clinical assessment; pump replacement surgery at the end of device battery life, typically every five to seven years; catheter revision procedures at a rate consistent with published complication literature; imaging for granuloma surveillance where clinically indicated; and management of any complications. Each of these components has identifiable market pricing and should be itemized separately in a defensible future care opinion. Defense review addresses whether the refill frequency, replacement interval, and complication rate assumptions are supported by the device specifications and the patient's clinical course.
- Yes. Dr. Dardashti accepts IDDS engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides. Review is available for the full scope of intrathecal pump-related issues — medical necessity, standard of care, causation of the underlying condition, device complication analysis, granuloma evaluation, baclofen withdrawal review, and future medical care — or for a defined subset of those issues depending on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope, available records, and availability.
Retain Dr. Dardashti for an Intrathecal Pump Case
Dr. Dardashti accepts intrathecal pump engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.