Nationwide Pain & Injury Medical Expert Witness
CRPS Expert Witness
Medical-legal review of Complex Regional Pain Syndrome — Budapest Criteria, causation, standard of care, spinal cord stimulation, and future medical care in personal injury and malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Condition
- Complex Regional Pain Syndrome (CRPS)
- Also Known As
- RSD — Reflex Sympathetic Dystrophy
- Types
- CRPS Type I / Type II
- Evaluation Areas
- Diagnosis, Causation, Standard of Care, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
CRPS in Litigation
Complex Regional Pain Syndrome is one of the most frequently litigated chronic pain conditions in personal injury and medical malpractice practice. Its combination of subjective pain complaints, complex diagnostic criteria, high lifetime treatment costs, and documented potential to develop after relatively minor trauma makes it a recurring subject of both plaintiff damages analysis and defense scrutiny.
CRPS litigation raises a distinct set of recurring issues: whether the diagnosis is supported by the clinical record and the Budapest Criteria; whether the precipitating event caused or materially aggravated the condition; whether the treatment rendered was medically necessary and consistent with the standard of care; and what future medical care is reasonably supported by the documented clinical trajectory. In cases where CRPS is refractory to conventional management, advanced interventions including spinal cord stimulation become components of the future care analysis and can significantly affect damages.
Expert review is case-specific. Opinions on diagnosis, causation, standard of care, and future care are grounded in the available medical records and the scope defined by retaining counsel — they do not presuppose an outcome for either party.
What Is Complex Regional Pain Syndrome?
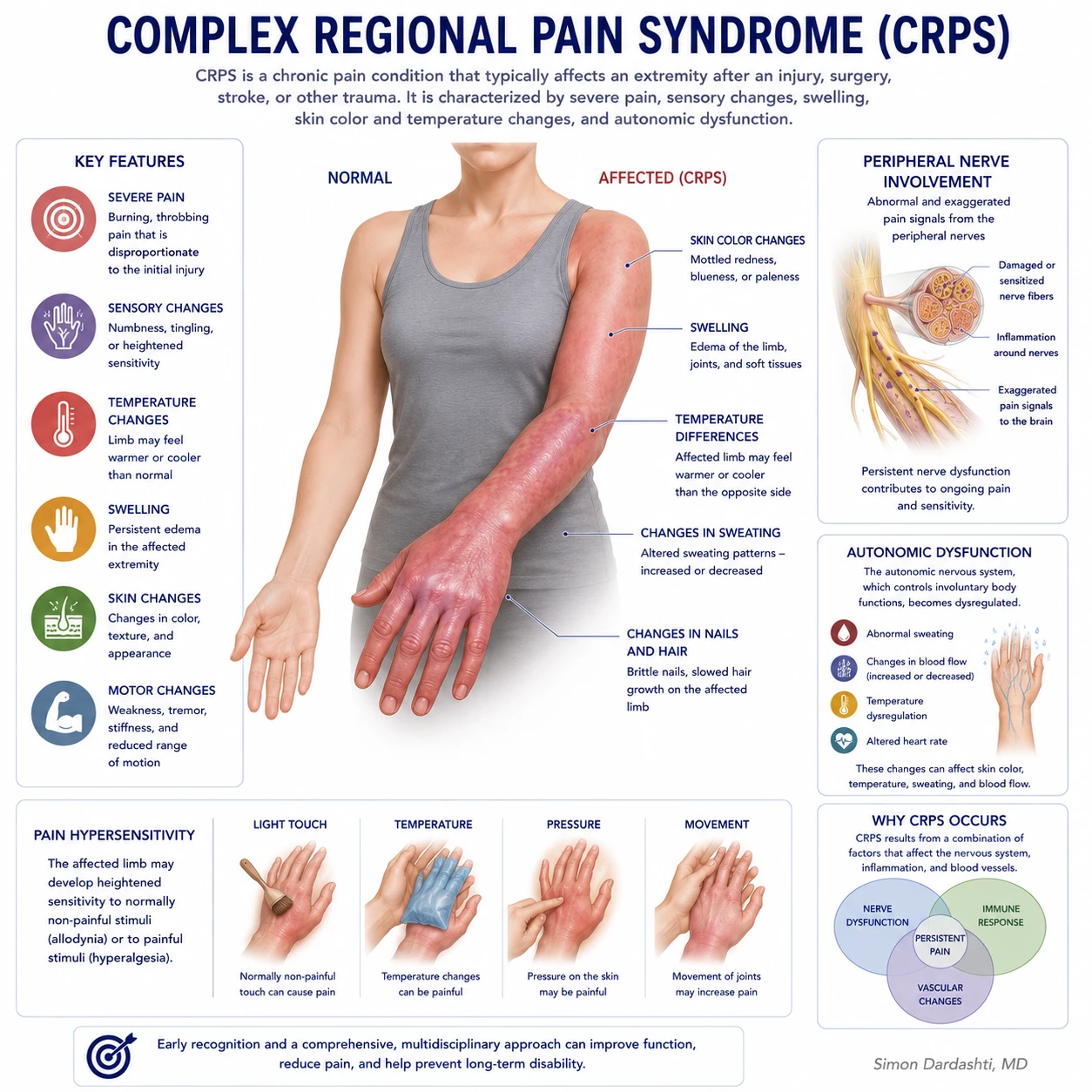
Complex Regional Pain Syndrome is a chronic neurological pain condition that typically affects a limb following trauma, surgery, or nerve injury. It is defined by pain that is disproportionate to the precipitating injury in both intensity and duration, combined with sensory, autonomic, and often motor and trophic changes in the affected limb. CRPS is classified into two types based on whether a peripheral nerve injury can be identified.
CRPS Type I — formerly called Reflex Sympathetic Dystrophy (RSD) — occurs without a confirmed peripheral nerve injury. The precipitating event may be a fracture, sprain, soft tissue injury, surgery, or in some cases a relatively minor trauma. Type I accounts for the majority of CRPS diagnoses in the clinical and litigation setting.
CRPS Type II — formerly called causalgia — follows a confirmed peripheral nerve injury. The clinical syndrome is identical to Type I; the distinction is that a specific nerve injury can be identified by history, physical examination, or electrodiagnostic testing. Type II CRPS arises in personal injury and malpractice matters involving direct nerve trauma, surgical nerve injury, and compression injuries.
The hallmark clinical features of CRPS include allodynia (pain produced by stimuli that do not normally cause pain, such as light touch), hyperalgesia (an exaggerated pain response to stimuli that do produce pain), temperature and skin color asymmetry between the affected and unaffected limb, abnormal sweating, edema, and in chronic cases, trophic changes including skin atrophy, abnormal hair and nail growth, and progressive joint and muscle changes. Motor dysfunction — including weakness, tremor, and in some cases fixed dystonia — may develop in later stages.
Common precipitating mechanisms include fractures (particularly distal radius fractures and tibial fractures), crush injuries, sprains, surgical procedures involving the extremities, intravenous catheter placement, and nerve injuries from any cause. A minority of cases occur without a clearly identifiable precipitating event. The severity of the precipitating injury does not predict the development or severity of CRPS — a feature of the condition that is frequently contested in litigation.
Budapest Diagnostic Criteria
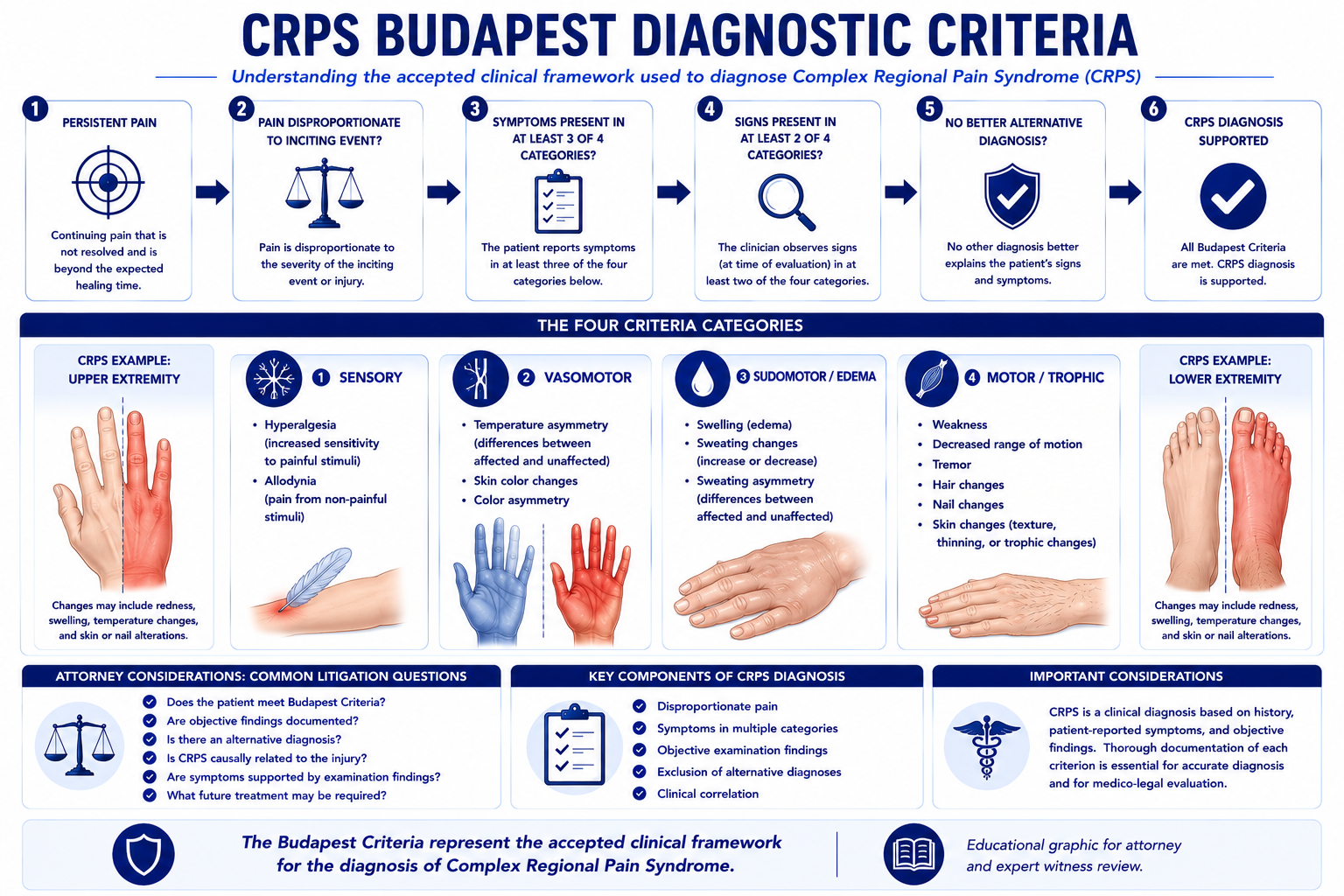
The Budapest Criteria are the internationally accepted diagnostic standard for CRPS, established following a 2003 consensus conference convened to replace the earlier and less specific International Association for the Study of Pain (IASP) criteria. Their adoption represented a significant shift in how CRPS is diagnosed in clinical practice and evaluated in the medical-legal setting.
For clinical diagnosis, the Budapest Criteria require that the patient report symptoms in at least three of four categories and that the examining clinician document objective signs on physical examination in at least two of those four categories. No other diagnosis should better account for the findings. The four diagnostic categories are:
- › Sensory — Reports of hyperalgesia (increased sensitivity to painful stimuli) and/or allodynia (pain from stimuli that do not normally cause pain, such as light touch or clothing contact)
- › Vasomotor — Reports of temperature asymmetry between the affected and unaffected limb, and/or skin color changes or asymmetry (mottling, erythema, pallor, or cyanosis)
- › Sudomotor / Edema — Reports of edema, sweating changes, or sweating asymmetry in the affected region
- › Motor / Trophic — Reports of decreased range of motion and/or motor dysfunction (weakness, tremor, or dystonia) and/or trophic changes (skin atrophy, abnormal nail or hair growth)
The distinction between reported symptoms and documented objective signs is clinically and legally significant. A clinician who documents only subjective complaints without recording the results of the physical examination has not established objective support for the Budapest Criteria in the medical record, regardless of whether the examination was actually performed. For the complete pain management examination methodology — including the range-of-motion, motor, sensory, and functional assessment components that establish the objective sign documentation underlying a Budapest Criteria analysis — see the article on how pain management experts objectively evaluate pain.
Several diagnostic studies may be obtained in the evaluation of CRPS but none is pathognomonic. Three-phase bone scintigraphy (bone scan) may show characteristic periarticular uptake in the affected extremity, particularly in the acute phase, but has limited sensitivity and specificity for CRPS. MRI may show soft tissue edema or trophic changes. Infrared thermography may document skin temperature asymmetry. Electrodiagnostic studies are relevant in cases where a peripheral nerve injury is suspected (CRPS Type II) but do not confirm or exclude CRPS Type I.
CRPS diagnosis is contested in litigation for several reasons: the reliance on clinical examination findings rather than objective biomarkers; the potential for symptom variability over time and across examination settings; the overlap between CRPS symptomatology and other pain conditions; and the practical reality that treating physicians may not systematically document findings in the four Budapest Criteria categories at each clinical encounter. Expert review addresses whether the aggregate clinical record — read as a whole and over time — supports the Budapest Criteria diagnosis, and whether the documentation adequately captures the objective findings required for that determination. For a comprehensive litigation guide to CRPS causation, Budapest Criteria documentation, expert challenges, and treatment projection, see the CRPS expert witness guide.
Causation Analysis
Causation analysis in CRPS matters addresses whether the clinical record supports a relationship between the subject event and the development or material aggravation of the condition. The analysis is multi-factor and case-specific.
- › Temporal relationship — CRPS typically develops within weeks to months of the precipitating event. Symptoms that appear immediately or within a clinically plausible timeframe following a documented injury are temporally consistent with causation. A significant unexplained gap between the injury and the onset of CRPS-consistent symptoms requires examination in the context of the full record.
- › Mechanism consistency — The mechanism of the subject injury and its consistency with known CRPS precipitants is assessed. Fractures, nerve injuries, crush mechanisms, and surgical trauma are recognized precipitants. The location of the injury and the distribution of the CRPS symptoms should be anatomically plausible.
- › Pre-existing conditions — The presence of prior pain conditions, prior injuries to the same extremity, or prior CRPS episodes is relevant to the causation analysis and may support an aggravation, rather than new-onset, causation opinion. Pre-existing conditions do not preclude causation but require specific analysis.
- › Clinical documentation from the relevant period — The treating records from the weeks and months following the subject event are the primary evidence base. The presence or absence of CRPS-consistent complaints, examination findings, and diagnostic workup during this period is central to the causation opinion.
- › Alternative explanations — The causation analysis addresses whether the clinical picture is better explained by an alternative diagnosis or by a condition unrelated to the subject event. Competing explanations supported by the record are part of the differential analysis, not a predetermined conclusion.
In personal injury matters involving pre-existing degenerative conditions, psychiatric history, or prior pain treatment, causation review addresses whether the subject event produced a new CRPS condition or materially aggravated and accelerated a pre-existing vulnerability. These are distinct causation theories with different implications for damages analysis.
Standard of Care Considerations
The standard of care for CRPS reflects the practice of a reasonably competent physician — whether primary care, orthopedic surgeon, or pain management specialist — encountering a patient with a clinical presentation consistent with CRPS. Core elements include recognition of the condition at an appropriate clinical stage, initiation of a multidisciplinary treatment approach, and appropriate referral when the condition exceeds the treating physician's area of expertise.
- › Early recognition — Current evidence supports early diagnosis and treatment initiation as the most important factor in CRPS outcome. Failure to recognize CRPS-consistent findings and initiate treatment — or to refer for pain management evaluation — within a clinically appropriate timeframe is a central standard of care issue in malpractice matters.
- › Multidisciplinary treatment — Published CRPS treatment guidelines support a multidisciplinary approach integrating physical rehabilitation, pharmacological management, psychological support, and interventional pain procedures. Reliance on a single treatment modality without addressing the full clinical picture may be a standard of care issue.
- › Physical and occupational therapy — Graded motor imagery, mirror visual feedback, and desensitization are evidence-based physical rehabilitation approaches for CRPS. Physical therapy that exacerbates rather than progressively mobilizes the affected limb, or failure to adapt the rehabilitation plan to the patient's clinical response, may be relevant to standard of care review.
- › Pharmacological management — Evidence-supported pharmacological agents for CRPS include calcium channel modulators (gabapentin, pregabalin), tricyclic antidepressants, bisphosphonates, NMDA receptor antagonists, and topical agents. Opioids have a limited evidence base for CRPS and are not a first-line treatment. The selection, dosing, and monitoring of pharmacological agents is a standard of care consideration in both malpractice and treatment necessity review.
- › Interventional procedures — Sympathetically targeted nerve blocks (stellate ganglion block for upper extremity CRPS, lumbar sympathetic block for lower extremity CRPS) are used both diagnostically and therapeutically. Their role in the treatment plan, the frequency with which they are performed, and the documentation of clinical response are all relevant to standard of care analysis.
Common Litigation Issues
CRPS cases present a recurring set of litigation issues that arise in both personal injury and medical malpractice contexts. These issues tend to cluster around diagnosis, causation, and the consequences of delayed or inadequate treatment.
- › Delayed diagnosis — CRPS is frequently unrecognized in the acute post-injury period, particularly when the initial treating clinician is an emergency physician or orthopedic surgeon. Delayed diagnosis — and the resulting delay in initiation of multidisciplinary treatment — is associated with worse clinical outcomes and is a central issue in CRPS malpractice claims.
- › Failure to refer to pain management — An orthopedic surgeon or primary care physician managing a post-traumatic or post-surgical patient who develops CRPS-consistent symptoms has a standard of care obligation to consider pain management referral when the condition is not responding to standard treatment. Failure to refer, or a significant delay in referral, is a recurring malpractice allegation.
- › Disputed Budapest Criteria documentation — Defense review frequently focuses on whether the treating physician's records document objective signs — not merely subjective complaints — in two or more Budapest Criteria categories at a contemporaneous examination. Incomplete or ambiguous documentation creates an evidentiary gap that expert review must address.
- › Exaggeration and malingering allegations — The absence of objective biomarkers for CRPS, combined with its potentially severe functional consequences, makes exaggeration or fabrication allegations common in defense review. Expert analysis addresses whether the clinical pattern — including the consistency of findings across multiple examinations by different providers — is consistent with genuine CRPS or with an alternative explanation.
- › Functional impairment disputes — CRPS can produce severe functional limitations including inability to use the affected extremity, work disability, and profound effects on activities of daily living. When these limitations are at issue in damages, expert review addresses whether the functional status is consistent with the documented clinical findings and treatment course. For the broader clinical methodology connecting functional findings to pain and suffering damages, see the article on pain management expert analysis after Gregory v. Chohan.
- › Disputed causation in minor trauma cases — When CRPS develops after a minor injury — a low-speed motor vehicle collision, a simple fracture, or a soft tissue sprain — the defense frequently disputes whether the injury was sufficient to cause the condition. Expert review addresses the established medical literature on CRPS precipitants and the specific clinical record in context.
Personal Injury Evaluation
Motor vehicle collisions are the most common personal injury context for CRPS claims. Extremity trauma — fractures, crush injuries, and nerve injuries — sustained in a collision can precipitate CRPS in the affected limb. Cases involving fractures of the distal radius (Colles fracture), tibial plateau, or ankle are among the most frequently litigated post-traumatic CRPS presentations. The temporal relationship between the documented fracture and the development of CRPS-consistent symptoms is typically a central element of the causation analysis.
In cases involving minor trauma, personal injury evaluation addresses the specific clinical documentation from the treating providers during the period between the injury and the CRPS diagnosis — including whether the post-injury clinical course, the pattern of symptom progression, and the physical examination findings are consistent with CRPS development following the mechanism of injury claimed.
Future medical care analysis in personal injury CRPS matters addresses the full anticipated treatment trajectory — including ongoing pharmacological management, periodic interventional procedures, physical and occupational therapy, and in appropriate cases the costs of advanced neuromodulation therapy. Future medical care projections are grounded in the documented clinical course and current treatment guidelines, not generic life care plan templates.
Medical Malpractice Evaluation
CRPS malpractice claims generally arise from delayed recognition, failure to refer, inadequate documentation, or substandard management of the condition once diagnosed. Expert review addresses whether the care provided by the treating physician met the applicable standard of care for a clinician in that specialty encountering a patient with a CRPS-consistent clinical presentation.
- › Post-surgical CRPS — recognition and disclosure — CRPS is a recognized surgical complication, particularly following orthopedic procedures on the extremities. A surgeon who encounters a post-operative patient with disproportionate pain, allodynia, and autonomic changes has an obligation to recognize the clinical picture, investigate it appropriately, and refer to pain management when indicated. Failure to recognize and disclose a surgical complication is a distinct standard of care issue from the initial decision to perform the surgery. Lumbar decompression surgery — including emergency decompression for cauda equina syndrome — carries the same post-surgical CRPS risk, and the pain management standard of care for post-surgical CRPS recognition and treatment applies independently to those cases alongside the neurosurgical standard of care for decompression timing.
- › Treatment delays and outcome consequences — The medical literature supports early, multidisciplinary treatment as the most significant predictor of CRPS outcome. When a delay in diagnosis or treatment is alleged to have resulted in a worse outcome — including progression to chronic refractory CRPS requiring SCS — the causation analysis addresses whether the delay, rather than the underlying condition, was the proximate cause of the outcome.
- › Documentation deficiencies — In CRPS malpractice cases, the absence of contemporaneous documentation of Budapest Criteria findings — symptoms reported and signs observed — may indicate that the clinical evaluation was inadequate, or that findings were present but not recorded. Either situation is potentially relevant to standard of care analysis.
- › Inappropriate treatment — Physical therapy protocols that are too aggressive for the stage and severity of CRPS — producing excessive mobilization pain and symptom exacerbation — can worsen outcomes and may be a standard of care issue. Similarly, prolonged sole reliance on opioid management without initiating multidisciplinary treatment reflects a departure from current guidelines.
Expert review is specific to pain management and anesthesiology. Opinions on surgical technique, surgical indication, or the orthopedic standard of care are outside this scope and require a specialty-matched expert.
Spinal Cord Stimulation and Advanced Treatment
Spinal cord stimulation is the most extensively studied advanced treatment for refractory CRPS and carries the strongest evidence base of any neuromodulation intervention for this condition. Randomized controlled trial evidence — including the landmark trials by Kemler et al. — has demonstrated clinically meaningful pain relief and quality of life improvement in patients with CRPS who have failed conservative management. SCS is listed as a recommended therapy in major published CRPS treatment guidelines.
SCS is considered for CRPS when the condition has proven refractory to an adequate trial of conservative and conventional interventional management — including physical therapy, pharmacological treatment with neuropathic agents, and sympathetically targeted procedures. The evaluation for SCS candidacy typically includes a psychological screening, a multidisciplinary review of the treatment course, and a trial stimulation period to assess pain relief and functional benefit before permanent implantation.
In the litigation context, SCS in CRPS cases arises in several ways. In personal injury damages analysis, it may be a component of future medical care projections when the clinical trajectory supports the likelihood of progression to refractory CRPS — the total cost of trial stimulation, permanent implantation, device replacement at approximately five to ten year intervals, and ongoing programming is substantial and materially affects damages calculations. In medical necessity disputes, the adequacy of the conservative treatment course preceding the SCS recommendation is a central issue.
Other advanced treatment modalities with evidence for refractory CRPS include ketamine infusion therapy, intrathecal drug delivery, and graded motor imagery intensive rehabilitation programs. The clinical appropriateness of any advanced treatment is evaluated against the documented treatment course and the current evidence base.
Expert Witness Review Process
CRPS cases require review of a defined set of records to support a complete medical-legal opinion. The specific records relevant to the engagement depend on the scope — diagnosis support, causation, standard of care, or future care — and are defined in consultation with retaining counsel. Typical records include:
- › Emergency department and initial treating records — Records from the period immediately following the precipitating event, documenting the initial injury, treatment, and early post-injury clinical course
- › Treating pain management records — Complete notes from the diagnosing and treating pain management physician, including initial evaluation, follow-up visits, procedure records, and pharmacological management notes
- › Orthopedic and surgical records — Operative reports, post-operative notes, and imaging interpretation from any surgery related to the precipitating event or performed after CRPS onset
- › Imaging studies — X-rays, MRI, CT, and where obtained, three-phase bone scintigraphy reports and raw images for the affected extremity and relevant spinal levels
- › Electrodiagnostic studies — Nerve conduction study and EMG reports where Type II CRPS or peripheral nerve injury is at issue
- › Physical and occupational therapy records — Treatment notes documenting the rehabilitation approach, the patient's response, and functional progress or limitations
- › Pre-existing medical records — Records predating the subject event to establish baseline health status, prior pain history, and prior treatment for the affected extremity
- › Prior IME and expert reports — Any prior independent medical examinations, functional capacity evaluations, or retained expert reports bearing on the diagnosis or causation issues
- › Deposition testimony — Testimony of the treating pain management physician, the claimant, and any other experts addressing the diagnosis, causation, or treatment course
Contact Expert Medical Services LLC with a brief case summary and a description of the available records. Engagements may address diagnosis, causation, standard of care, or future medical care projections and can be structured to address one or more of these issues within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Spinal Cord Stimulation
SCS is the established advanced treatment for refractory CRPS — necessity, cost, and causation.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California.
Causation Analysis
Linking the mechanism of injury to a CRPS diagnosis and treatment course.
Future Medical Care Review
Long-term cost projections for CRPS treatment, SCS, and ongoing pain management.
Medial Branch Block
Expert review of MBB medical necessity, standard of care, and the diagnostic pathway to RFA.
Radiofrequency Ablation
Expert review of RFA medical necessity, standard of care, and the diagnostic pathway from medial branch blocks.
Amputation & Phantom Limb Pain
Amputation can precipitate CRPS Type II — neuropathic pain, residual limb pain, and phantom limb overlap.
Arizona Pain Management Expert Witness
CRPS and complex pain expert review for Arizona personal injury litigation.
Florida Pain Management Expert Witness
CRPS and complex pain expert review for Florida personal injury and medical malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for CRPS interventions — spinal cord stimulation, intrathecal pump, and sympathetic blocks.
Standard of Care Analysis
Standard of care analysis for CRPS diagnosis, treatment escalation, and interventional pain management.
FAQ
CRPS — Common Attorney Questions
- Complex Regional Pain Syndrome is a chronic neurological pain condition that typically affects one or more limbs following trauma, surgery, or nerve injury. It is characterized by pain that is disproportionate to the precipitating injury in intensity or duration, combined with sensory changes such as allodynia and hyperalgesia, autonomic dysfunction including temperature and skin color changes, and often motor and trophic changes. CRPS is classified into two types: Type I, which occurs without a confirmed nerve injury and was formerly called Reflex Sympathetic Dystrophy (RSD); and Type II, which follows a confirmed peripheral nerve injury and was formerly called causalgia. Both types share the same diagnostic criteria and produce the same clinical syndrome.
- The Budapest Criteria are the internationally accepted diagnostic standard for CRPS, established following a 2003 consensus conference to replace the earlier and less specific IASP criteria. For clinical diagnosis, the patient must report symptoms in at least three of four categories — sensory (hyperalgesia or allodynia), vasomotor (temperature asymmetry or skin color changes), sudomotor or edema (sweating changes or edema), and motor or trophic (decreased range of motion, weakness, tremor, dystonia, or trophic changes) — and the examining clinician must document objective signs in at least two of those four categories on physical examination. No other diagnosis should better explain the findings. For research purposes, the criteria are slightly more stringent, requiring signs in three of four categories. Because the Budapest Criteria depend on contemporaneous clinical examination findings, the completeness and quality of the treating physician's records is a central evidentiary issue in CRPS litigation.
- CRPS Type I occurs without a confirmed peripheral nerve injury. The precipitating event may be a fracture, sprain, surgery, immobilization, or in some cases relatively minor trauma. CRPS Type II follows a confirmed peripheral nerve injury — the clinical syndrome is identical, but a specific nerve injury can be identified by history, physical examination, or electrodiagnostic testing. In litigation, the Type I/Type II distinction matters for causation analysis, for the question of whether electrodiagnostic evaluation was obtained and interpreted appropriately, and for standard of care analysis in cases where a nerve injury was or should have been identified.
- Causation review addresses whether the clinical record supports a relationship between the subject event and the development or aggravation of CRPS. The analysis considers the temporal relationship between the precipitating event and the onset of CRPS-consistent symptoms; the mechanism of injury and its consistency with known CRPS precipitants; the pre-existing medical history including any prior pain conditions or prior injuries to the same extremity; the contemporaneous clinical documentation from the period between the event and the CRPS diagnosis; and whether alternative explanations for the clinical picture are supported by the record. Causation review is case-specific and does not presuppose an outcome for either party.
- Yes. CRPS is documented in the medical literature as a condition that can develop following injuries that would otherwise be expected to resolve — including minor fractures, sprains, contusions, and venipuncture. The severity of the precipitating injury does not predict the likelihood or severity of CRPS. The disproportionate pain response following minor trauma is one of the defining clinical features of the condition and one of the most contested aspects of causation analysis in CRPS litigation, where the defense frequently argues that the injury was too minor to explain the alleged impairment. The medical literature, including the Budapest Criteria framework, addresses this directly.
- Yes. Post-surgical CRPS is a recognized complication of surgery — particularly surgery involving the extremities — and arises in both personal injury and medical malpractice contexts. In personal injury matters, post-surgical CRPS may follow orthopedic or other surgery performed to treat a traumatic injury, raising questions about whether the original accident or the surgery contributed to the condition. In malpractice matters, the question may be whether post-surgical CRPS was recognized at an appropriate stage of the clinical course, whether a timely referral to a pain management specialist was made, and whether earlier recognition and treatment would have affected outcome.
- Spinal cord stimulation is considered for CRPS when the condition is refractory to conservative and conventional interventional management — including physical therapy, pharmacological treatment with neuropathic agents, and sympathetically targeted procedures such as stellate ganglion or lumbar sympathetic blocks. Randomized controlled trial evidence supports SCS for CRPS, and it is listed as a recommended therapy in published treatment guidelines. In litigation, SCS may arise as a future care element in personal injury damages analysis or as a past treatment whose necessity and causation is disputed. The cost of SCS — including trial stimulation, permanent implantation, programming, and periodic device replacement — is a significant component of future medical care projections in high-value CRPS matters.
- Future medical care review in CRPS addresses the long-term treatment needs supported by the clinical record — including the diagnosis, the treatment course to date, the clinical trajectory, and the patient's functional status. Reasonable future care projections may include ongoing pharmacological management, periodic interventional procedures, physical and occupational therapy, and in refractory cases, spinal cord stimulation with associated device replacement costs. The projection is case-specific and is grounded in the clinical record, not a standardized template. Defense review of a plaintiff life care plan addresses whether proposed care items are medically supported by the documented clinical course, appropriately priced, and consistent with current treatment guidelines.
- Key records include the complete treating pain management notes, emergency department and initial treating records from the period immediately following the precipitating event, pre-existing medical records to establish baseline, imaging studies (X-ray, MRI, and where obtained, three-phase bone scintigraphy), electrodiagnostic studies if a nerve injury is at issue, physical and occupational therapy records, pharmacological and interventional treatment records documenting the clinical response to each treatment modality, functional capacity evaluation reports, and — where the diagnosis has been contested — prior independent medical examination reports and expert opinions. The completeness and contemporaneity of the clinical documentation is frequently the central evidentiary issue in CRPS litigation.
- Malpractice review in CRPS matters addresses whether the care provided met the applicable standard for a pain management or treating physician. Common issues include whether CRPS was recognized at an appropriate point in the clinical course, whether treatment was initiated within a timeframe consistent with current guidelines, whether a timely referral to a pain management specialist was made, and whether clinical documentation adequately captured the findings required for Budapest Criteria diagnosis. In post-surgical CRPS cases, additional issues include whether the complication was recognized and disclosed appropriately, and whether the management of the condition was consistent with standard pain management practice. Opinions are specific to pain management; orthopedic or neurosurgical standard of care is outside this scope.
Retain a CRPS Expert for Your Case
Dr. Dardashti accepts CRPS engagements for both retaining parties in state and federal courts nationwide. Contact Expert Medical Services LLC to discuss case scope and availability.