Nationwide Pain & Injury Medical Expert Witness
Peripheral Nerve Injury Expert Witness
Expert evaluation of peripheral nerve injury — causation, electrodiagnostic findings, CRPS Type II, neuroma formation, standard of care, and future medical care in complex personal injury and malpractice litigation.
Request AvailabilityCredentials & Qualifications
- Condition
- Peripheral Nerve Injury
- Also Known As
- Traumatic Neuropathy, Mononeuropathy
- Specialty
- Pain Management & Anesthesiology
- Evaluation Areas
- Causation, Standard of Care, Electrodiagnostics, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Peripheral Nerve Injury in Medical-Legal Review
Peripheral nerve injury encompasses damage to any nerve outside the brain and spinal cord — the motor and sensory nerves that connect the central nervous system to the muscles, skin, and organs of the body. The consequences range from transient sensory changes and conduction block that resolve over weeks, to permanent neuropathic pain, sensory loss, and motor deficit requiring long-term treatment and, in refractory cases, advanced neuromodulation. Peripheral nerve injury is among the most frequently contested diagnoses in personal injury and medical malpractice litigation because objective documentation requires electrodiagnostic evaluation, and clinical findings require specialist interpretation to distinguish genuine structural nerve injury from pain without an identified nerve injury mechanism.
In the litigation context, peripheral nerve injury arises across a broad range of case types. In personal injury matters, it follows lacerations, crush injuries, traction injuries, and compressive injuries from occupational or accidental mechanisms. In medical malpractice matters, it arises as a surgical complication — a nerve damaged during an operative procedure. In amputation cases, peripheral nerve injury at the time of amputation, neuroma formation at the residual limb, and the pre-amputation nerve injury history all affect the post-amputation pain syndrome and future care analysis.
Expert review is grounded in the clinical record, the available electrodiagnostic studies, and the scope of questions defined by retaining counsel. Opinions are case-specific and do not presuppose an outcome for either party.
What Is Peripheral Nerve Injury?
The peripheral nervous system consists of the nerve fibers that carry motor signals from the spinal cord to muscles, sensory signals from the skin, joints, and viscera to the spinal cord, and autonomic signals that regulate involuntary functions. Each peripheral nerve is composed of axons — the conducting fibers — surrounded by a layered connective tissue architecture: the endoneurium surrounds individual axons, the perineurium bundles axons into fascicles, and the epineurium surrounds the entire nerve trunk. This connective tissue architecture is critical to the classification of injury severity and the prognosis for recovery.
Peripheral nerve injury produces clinical effects that depend on which nerve is injured, the location of injury along the nerve, and the degree of structural disruption. Motor effects include weakness or paralysis of the muscles supplied by the affected nerve. Sensory effects include hypoesthesia (reduced sensation), paresthesia (abnormal sensation such as tingling or pins and needles), dysesthesia (unpleasant abnormal sensation), and neuropathic pain in the distribution of the affected nerve. Autonomic effects — skin color and temperature changes, sweat abnormalities, and trophic skin and nail changes — occur in injuries to nerves with significant autonomic fiber content, and when present can suggest the development of Complex Regional Pain Syndrome.
The neuropathic pain of peripheral nerve injury is clinically distinct from the nociceptive pain of tissue injury. It has a burning, electric, or shooting quality; it is often present at rest without mechanical provocation; it may be triggered or worsened by normally non-painful stimuli (allodynia) or produce exaggerated responses to normally painful stimuli (hyperalgesia); and it may extend beyond the anatomical territory of the injured nerve as central sensitization develops over time. These features — particularly allodynia and the disproportionate pain response — are among the most frequently contested aspects of peripheral nerve injury presentation in litigation.
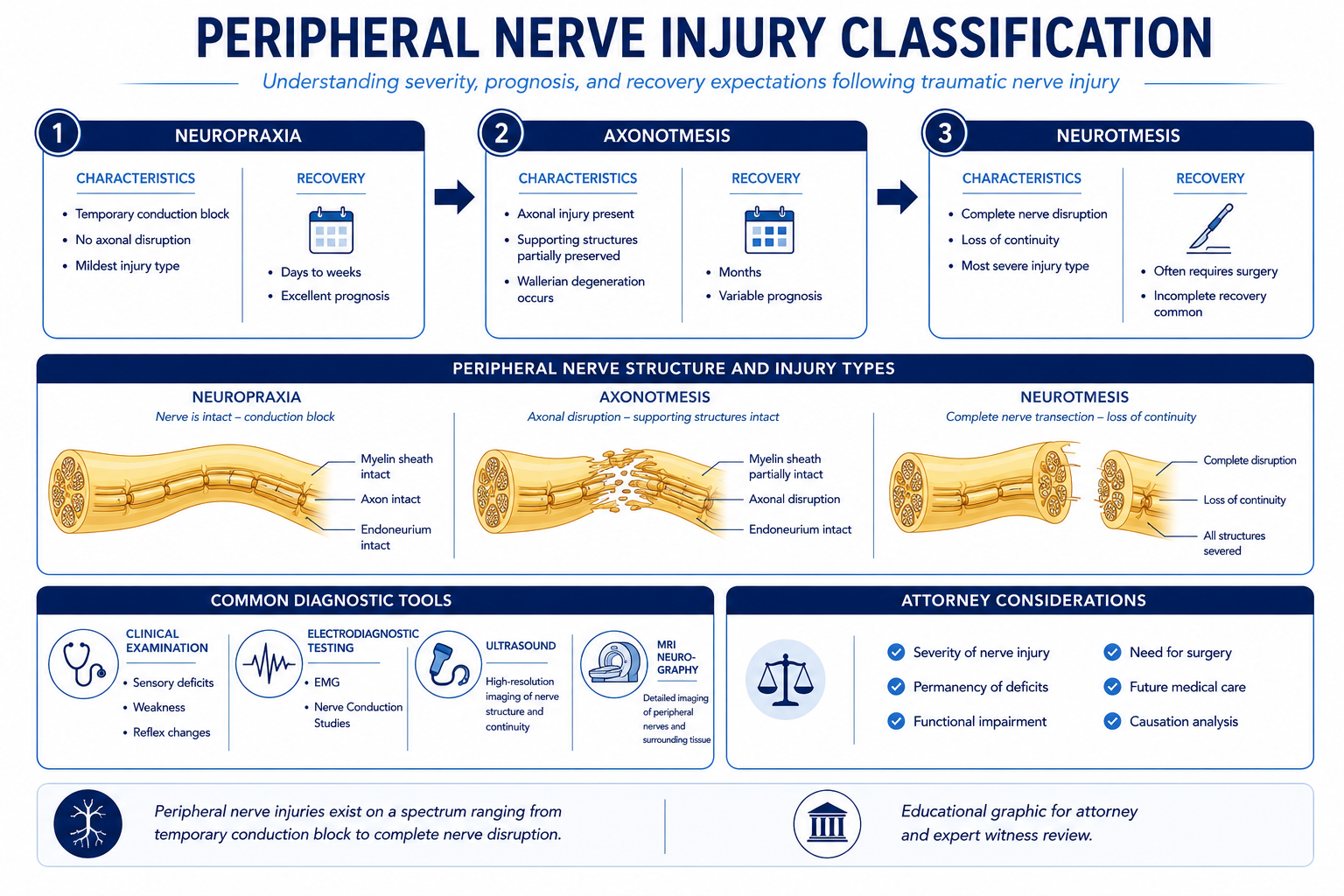
Nerve Injury Classification: Neuropraxia, Axonotmesis, Neurotmesis
Peripheral nerve injuries are classified according to the degree of structural disruption to the nerve. The Seddon classification — the most commonly used framework in clinical and medico-legal contexts — identifies three grades, each with distinct mechanisms, electrodiagnostic correlates, prognoses, and treatment implications:
- › Neuropraxia — the mildest injury, involving disruption of conduction without structural damage to the axon or its connective tissue envelope. Neuropraxia is produced by compression, ischemia, or mild stretch, and results in a conduction block — the nerve cannot transmit signals across the injured segment, producing weakness and sensory change in the distribution of the affected nerve. The axon remains structurally intact, and recovery occurs as the conduction block resolves, typically over days to weeks. Neuropraxia does not produce denervation changes on EMG because the axon has not degenerated. Nerve conduction studies show reduced amplitude or conduction block across the injury site but normal findings distal to the injury. Full recovery is the expected outcome, and the prognosis for recovery is good. In litigation, neuropraxia is relevant in cases of transient nerve compression — compartment syndrome, tourniquet injury, cast compression — and in the early period following crush or traction injuries before the extent of axon damage is established.
- › Axonotmesis — a more severe injury involving disruption of the axon with preservation of the surrounding connective tissue architecture — the endoneurial tubes remain intact. Axonotmesis is produced by more severe compression, traction, or crush, and results in Wallerian degeneration — the axon distal to the injury site degenerates because it is no longer in continuity with the nerve cell body. On EMG, fibrillation potentials and positive sharp waves — signs of active denervation — appear in the affected muscles 10 to 21 days after injury. On NCS, amplitude is reduced distal to the injury once Wallerian degeneration is complete, approximately 7–10 days post-injury. Because the endoneurial tubes are preserved, axonal regrowth can proceed along the intact scaffold at approximately 1–3 mm per day from the injury site. Recovery occurs over months, is dependent on the distance from the injury to the target muscle or sensory end organ, and may be incomplete. In litigation, axonotmesis is the most common significant nerve injury grade seen following crush injuries, traction injuries, and compressive injuries of moderate severity.
- › Neurotmesis — the most severe injury, involving complete structural disruption of the nerve — the axon, the endoneurium, the perineurium, and the epineurium are all divided. Neurotmesis is produced by laceration, high-energy traction, avulsion, or complete crush. It results in complete denervation of all structures supplied by the affected nerve, with no spontaneous recovery — axonal regrowth cannot occur because there is no intact connective tissue scaffold to guide regeneration. Surgical repair — nerve grafting or direct primary repair — is required to provide any possibility of functional recovery, and results are variable and often incomplete, particularly for nerves with long distances to their target muscles. On EMG and NCS, the findings are those of complete axon loss — absent compound motor and sensory action potentials, active denervation without reinnervation on serial studies. In litigation, neurotmesis is the expected finding in sharp laceration injuries and in avulsion injuries, and is the grade that most commonly produces permanent residual deficit and requires the most extensive future care projections.
The Sunderland classification expands Seddon's three grades into five degrees, subdividing axonotmesis into three degrees based on the specific connective tissue layers involved, which provides more granular prognostic information. In medical-legal review, the Sunderland classification is relevant when the electrodiagnostic and clinical record are being interpreted for prognosis — particularly in cases where spontaneous partial recovery is documented and its extent needs to be characterized.
Mechanisms of Traumatic Nerve Injury
The mechanism of peripheral nerve injury is clinically and medico-legally significant because it determines the expected injury grade, the anatomical nerve distribution that should be affected, the expected electrodiagnostic timeline, and the prognosis. Major traumatic mechanisms include:
- › Laceration — sharp instrument injury, glass laceration, machinery contact, or projectile injury that physically divides one or more peripheral nerves. Lacerations are the most common cause of neurotmesis. The extent of nerve disruption depends on the sharpness of the instrument and the anatomical depth of the wound. In the upper extremity, median and ulnar nerve lacerations at the wrist or forearm are common; radial nerve lacerations occur in spiral fractures of the humerus. In the lower extremity, sciatic nerve, peroneal nerve, and tibial nerve injuries are seen in high-energy trauma. Sharp laceration injuries typically require surgical exploration and repair.
- › Crush injury — compressive force applied to a limb segment that damages nerve, blood vessels, and muscle. Crush injuries typically produce axonotmesis, though severe crushing force can cause neurotmesis. The zone of nerve injury may be extensive, complicating surgical repair. Crush injuries are common in industrial accidents, vehicle rollover, and machinery entrapment incidents. Crush injury to a nerve in a confined anatomical compartment — such as the median nerve in the carpal tunnel or the sciatic nerve in the posterior thigh — may also produce compartment syndrome, which adds a vascular and ischemic component to the nerve injury mechanism.
- › Traction injury — stretching force applied to a nerve or nerve plexus, produced by mechanisms including brachial plexus traction in shoulder dystocia or high-energy upper extremity trauma, lumbosacral plexus injury from pelvic fractures, or sciatic nerve stretch from posterior hip dislocation. Traction injuries produce varying degrees of nerve disruption depending on the magnitude of the stretching force. Root avulsion — in which a nerve root is torn from the spinal cord — is the most severe form of traction injury and is not amenable to repair. Brachial plexus traction injuries are a recognized complication of shoulder surgery in malpractice matters involving positioning-related nerve injuries.
- › Compression — sustained pressure on a nerve producing ischemia and conduction block. Acute compression injuries arise from casting, tourniquet use, or prolonged positioning (compartment syndrome, position-related nerve compression in surgery). Chronic entrapment neuropathies — carpal tunnel syndrome (median nerve), cubital tunnel syndrome (ulnar nerve at the elbow), fibular tunnel syndrome (peroneal nerve), or tarsal tunnel syndrome (tibial nerve) — arise from repetitive mechanical compression at anatomically narrow nerve passageways and can be aggravated by occupational activities, traumatic swelling, or systemic conditions. In litigation, entrapment neuropathies may arise as occupational disease claims, as sequelae of trauma that narrows the anatomical tunnel, or as aggravation of a pre-existing sub-clinical entrapment.
- › Fracture-associated nerve injury — peripheral nerves run in close anatomical proximity to bones and may be injured by fracture fragment displacement, by the initial traumatic force that produced the fracture, or by subsequent swelling and compartment pressure. The radial nerve in the spiral groove of the humerus (Holstein-Lewis fracture), the peroneal nerve at the fibular neck, and the median nerve in supracondylar humerus fractures are classic fracture-nerve injury associations. Fracture-associated nerve injury may be identified at initial presentation or may become apparent in the subacute period as swelling and hemorrhage evolve. The timing of nerve injury relative to the fracture event — and whether it was present at initial evaluation — can be a significant issue in malpractice matters involving fracture management.
Electrodiagnostic Testing — EMG and Nerve Conduction Studies
Electrodiagnostic testing — comprising nerve conduction studies (NCS) and electromyography (EMG) — is the primary objective tool for confirming peripheral nerve injury, characterizing its severity, localizing its anatomical site, and tracking recovery over time. In the medico-legal context, the quality, completeness, and interpretation of the electrodiagnostic record is frequently a central issue.
Nerve conduction studies apply a surface electrical stimulus to a peripheral nerve and measure the resulting signal at a downstream recording site. Motor NCS measures the compound muscle action potential — the summed electrical activity of all muscle fibers depolarized by the stimulus — and provides information about both conduction velocity (affected by demyelination) and amplitude (affected by axon loss). Sensory NCS measures the sensory nerve action potential, which is often more sensitive for early demyelinating or axon loss changes. Conduction block — a finding where the amplitude of the signal is substantially reduced with proximal versus distal stimulation — identifies a focal point of nerve injury and may indicate neuropraxia or early axonotmesis. F-wave and H-reflex testing can evaluate proximal nerve segments and nerve roots that cannot be directly stimulated with surface techniques.
Electromyography inserts a small recording electrode into muscle tissue and evaluates the electrical activity of individual motor units at rest and during voluntary contraction. In a denervated muscle — one that has lost its nerve supply following axon loss — spontaneous electrical activity appears in the form of fibrillation potentials and positive sharp waves. These denervation potentials do not appear immediately after nerve injury; they develop 10 to 21 days post-injury as Wallerian degeneration progresses. Their absence in the first two weeks after injury does not exclude axonotmesis or neurotmesis. Reinnervation potentials — polyphasic motor units of abnormal duration and amplitude — develop later as regenerating axons reestablish contact with muscle fibers and provide evidence of nerve recovery.
The timing of electrodiagnostic testing relative to the injury is critical to interpretation. A study performed too early — within 10 days of an axonotmesis or neurotmesis — may be falsely reassuring because Wallerian degeneration is not yet complete and denervation potentials have not yet appeared. A complete electrodiagnostic evaluation at the appropriate time post-injury, performed by a qualified physiatrist or neurologist using standardized technique with adequate nerve survey, is the evidentiary standard in peripheral nerve injury cases.
In the litigation context, expert review of the electrodiagnostic record addresses: whether the study was technically adequate; whether the nerve survey was complete for the clinical question; whether the findings are consistent with the mechanism and timeline of the alleged injury; whether the interpretation was correct; and whether serial studies were obtained at appropriate intervals to track recovery. Incomplete nerve surveys — where only a few nerves were tested rather than a comprehensive bilateral comparison — are a common quality concern in peripheral nerve injury cases. For the broader pain management evaluation methodology in which electrodiagnostic findings are integrated with clinical examination, range-of-motion assessment, validated functional instruments, and symptom validity testing, see the article on how pain management experts objectively evaluate pain.
Surgical Nerve Injury and Neuroma Formation
Iatrogenic peripheral nerve injury — nerve damage occurring as a complication of surgery — is among the most significant categories of peripheral nerve injury in the medical malpractice context. Peripheral nerves may be injured during surgery by direct division, retraction injury, compression by a retractor, thermal injury from electrocautery, ischemia from vascular compromise, or entrapment in suture or hardware. The anatomical proximity of major peripheral nerves to operative fields means that nerve injury is a recognized complication risk for many surgical procedures — but a recognized risk is not the same as an acceptable departure from the standard of care.
Common surgical nerve injuries include: the radial nerve in procedures involving the posterior humerus; the ulnar nerve in elbow procedures; the median nerve in carpal tunnel or forearm procedures; the common peroneal nerve in knee or proximal fibula procedures; the lateral femoral cutaneous nerve in anterior hip approaches; the femoral nerve in retractor-related injury during pelvic or retroperitoneal surgery; and the sciatic nerve in posterior hip arthroplasty. In each case, the question is whether the nerve injury was a consequence of a recognized procedural risk or whether it resulted from a departure from appropriate surgical technique or intraoperative decision-making.
Neuroma formation occurs when a peripheral nerve is completely or severely divided and the proximal end attempts regeneration without a distal pathway — either because the distal stump is absent (amputation), misaligned (laceration without repair), or blocked by scar tissue (inadequate surgical repair or post-injury fibrosis). The regenerating nerve sprouts form a disorganized ball of nerve fibers and connective tissue at the nerve end — the neuroma — that is exquisitely sensitive to mechanical stimulation. Pressure on the neuroma, vibration, or movement in the area produces severe local pain and may trigger radiating neuropathic pain in the distribution of the affected nerve.
Neuroma pain is a distinct clinical problem that requires specific treatment — it is not treated by the same pharmacological and interventional approaches used for radicular or facet-mediated pain. Neuroma management options include pharmacological neuropathic agents, targeted perineural injections, surgical excision with nerve grafting or implantation of the nerve end into muscle or bone, and in refractory cases, peripheral nerve stimulation or spinal cord stimulation. In litigation, failure to recognize neuroma formation as a distinct pain generator — and failure to obtain appropriate evaluation and treatment — is a standard of care consideration. In amputation cases, neuromas at the residual limb nerve ends are a recognized and treatable contributor to residual limb pain that is distinct from phantom limb pain.
CRPS Type II and Peripheral Nerve Injury
Complex Regional Pain Syndrome Type II — historically called causalgia — is a specific complication of peripheral nerve injury in which the full CRPS clinical syndrome develops in the distribution of the injured nerve. The Budapest Criteria for CRPS require documented symptoms in at least three of four clinical categories (sensory changes including allodynia or hyperalgesia; vasomotor changes including temperature asymmetry or skin color abnormality; sudomotor changes or edema; motor or trophic changes including decreased range of motion, weakness, tremor, or dystonia) with objective signs in at least two categories, in the context of a confirmed peripheral nerve injury. CRPS Type II is distinguished from CRPS Type I by the presence of the confirmed nerve injury — the clinical syndrome is otherwise identical.
The development of CRPS Type II following a peripheral nerve injury materially elevates the complexity and damages implications of the underlying case. CRPS is a chronic, often refractory condition that does not resolve with simple treatment of the nerve injury itself. It requires a distinct, multi-modal treatment approach, may require advanced neuromodulation including spinal cord stimulation, and carries long-term functional and vocational consequences that generate substantial future care costs. In personal injury matters, the progression from peripheral nerve injury to CRPS Type II is a recognized and foreseeable complication that substantially increases the damages trajectory.
The distinction between a peripheral nerve injury with neuropathic pain and a full CRPS Type II diagnosis is clinically important and is not always made correctly in the treating record. A treating physician who evaluates a patient with post-traumatic neuropathic pain in a peripheral nerve distribution but does not apply the Budapest Criteria framework, does not document the presence or absence of vasomotor, sudomotor, and trophic signs, and does not apply the CRPS Type II diagnosis when it is clinically supported, may be underdiagnosing and undertreating a patient's condition. In expert review, the question is whether the clinical record contains sufficient documentation to apply or rule out the Budapest Criteria, and whether the treatment approach was consistent with a CRPS diagnosis when one was warranted.
In malpractice cases where a surgical nerve injury leads to CRPS Type II, the analysis addresses both the surgical standard of care (the nerve injury itself) and the post-injury pain management standard of care (whether CRPS Type II was recognized and appropriately managed). These are separate standards requiring separate expert input — surgical standard of care and pain management standard of care are distinct specialties.
Medical Necessity and Treatment Escalation
Medical necessity review in peripheral nerve injury cases evaluates whether the treatments rendered or proposed are consistent with recognized clinical practice for the documented injury and pain pattern. Treatment follows a graduated escalation from conservative management through interventional procedures and, in refractory cases, advanced neuromodulation.
- › Pharmacological management — neuropathic pain agents form the first-line pharmacological approach for peripheral neuropathic pain. Calcium channel modulators (gabapentin, pregabalin) and tricyclic antidepressants (amitriptyline, nortriptyline) have established evidence for neuropathic pain of peripheral nerve origin. Serotonin-norepinephrine reuptake inhibitors (duloxetine) are also indicated for peripheral neuropathic pain. The rationale for the specific medications selected, the documented clinical response, and the basis for medication changes are elements of the medical necessity and standard of care analysis in treatment-intensive cases.
- › Physical and occupational therapy — Desensitization therapy, graded sensory re-education, and neuromuscular rehabilitation are important components of peripheral nerve injury management. Physical therapy addresses motor recovery and functional restoration; occupational therapy addresses adaptive function and activities of daily living. The adequacy and duration of therapeutic effort is a recurring issue in cases where the defense argues that the patient failed to pursue adequate conservative management before escalating to interventional care.
- › Targeted nerve blocks and injections — Perineural injections, peripheral nerve hydrodissection, and regional nerve blocks may be used for diagnostic and therapeutic purposes in peripheral nerve injury. In neuroma cases, targeted perineural injections with local anesthetic and steroid can provide temporary diagnostic relief and therapeutic benefit. The documentation of each procedure — the specific nerve targeted, the approach, the response, and the basis for repeat injections — is subject to medical necessity review.
- › Surgical management — Nerve decompression, primary nerve repair, nerve grafting, neuroma excision, and nerve transfer are surgical options depending on the injury type and the timing of intervention. The indications for surgical intervention, the timing, and the approach are within the scope of peripheral nerve surgery or neurosurgery — not pain management. However, post-operative pain management following nerve surgery is within the pain management scope, and the adequacy of post-surgical pain management is a standard of care issue in cases where neuropathic pain persists following attempted surgical repair.
- › Escalation criteria for neuromodulation — Spinal cord stimulation or peripheral nerve stimulation is considered when the peripheral neuropathic pain is refractory to an adequate documented trial of conservative and interventional management. The adequacy of the conservative care trial — specifically whether the appropriate pharmacological and physical therapy approaches have been attempted with documented clinical responses — is the threshold criterion for medical necessity of neuromodulation. A treating physician who proceeds to neuromodulation without documenting failure of appropriate conservative care faces a medical necessity challenge regardless of the genuine severity of the patient's pain.
Spinal Cord Stimulation for Refractory Neuropathic Pain
Spinal cord stimulation is an established treatment option for refractory peripheral neuropathic pain when the pain distribution and quality are appropriate for the modality and when conservative management has failed. SCS delivers electrical impulses through epidurally placed leads to the dorsal columns of the spinal cord, modulating pain signaling before it reaches consciousness. The mechanism is effective for neuropathic pain with a dermatomal or peripheral nerve distribution that can be covered by SCS paresthesia or sub-perception stimulation.
For peripheral nerve injury specifically, SCS is most clearly supported when the neuropathic pain has a radicular or dermatomal distribution corresponding to a spinal cord level that can be targeted by thoracic or cervical lead placement. Focal peripheral nerve pain — such as pain in the distribution of the ulnar nerve at the wrist — may be better addressed by peripheral nerve stimulation (direct stimulation of the injured nerve) rather than spinal cord stimulation, though SCS remains an option when peripheral nerve stimulation is not technically feasible. CRPS Type II arising from peripheral nerve injury is a well-supported SCS indication with randomized trial evidence, and the CRPS Type II pathway to SCS carries a stronger evidence base than SCS for traumatic peripheral neuropathic pain alone.
The pre-implant evaluation requirements for SCS in peripheral nerve injury cases are the same as for all SCS indications: documented failure of appropriate conservative management, a psychological screening evaluation by a qualified mental health provider, and a successful trial stimulation period with contemporaneous documentation of pre-trial and post-trial pain scores demonstrating at least 50% improvement. The presence of each of these elements — and the quality of their documentation — is subject to medical necessity review.
In personal injury damages analysis, when a traumatic peripheral nerve injury has produced refractory neuropathic pain and the clinical record supports a trajectory toward SCS, the future care projection includes the trial stimulation procedure, permanent implantation, device-specific battery replacement cycles, revision procedures at published complication rates, and ongoing programming visits. The aggregate SCS cost over the patient's life expectancy is a significant component of damages in high-value peripheral nerve injury and CRPS Type II cases. Cases involving cauda equina syndrome — a polyradicular nerve root compression injury — follow the same SCS eligibility framework for post-decompression neuropathic pain, with the important distinction that perineal and perianal pain from sacral nerve root injury may require sacral-targeted stimulation approaches rather than standard thoracic lead placement.
Standard of Care Considerations
The standard of care for peripheral nerve injury pain management addresses the obligations of the pain management physician who evaluates and treats a patient with neuropathic pain from a documented or suspected peripheral nerve injury. Expert review in peripheral nerve injury cases addresses pain management standard of care — it does not address surgical technique, orthopedic reduction methods, or the neurosurgical standard of care for nerve repair, which require different specialists.
- › Electrodiagnostic evaluation — When a pain management physician evaluates a patient with neuropathic pain in a peripheral nerve distribution, obtaining or reviewing electrodiagnostic studies — or ordering them if they have not been performed — is a standard of care element. Treating neuropathic pain without confirming the diagnosis and characterizing the nerve injury with electrodiagnostics is a quality concern, particularly when the distinction between peripheral nerve injury, radiculopathy, and CRPS Type II affects the treatment approach.
- › CRPS Type II recognition — A pain management physician evaluating a patient with confirmed peripheral nerve injury has a standard of care obligation to apply the Budapest Criteria framework and document the presence or absence of the clinical features required for a CRPS Type II diagnosis. Failure to apply the Budapest Criteria, failure to document the relevant physical examination findings, and failure to diagnose CRPS Type II when it is clinically present can result in undertreatment and may constitute a standard of care deviation — particularly when early aggressive treatment of CRPS is known to affect long-term outcomes.
- › Referral obligations — A primary care physician, orthopedic surgeon, or other treating physician who encounters a patient with neuropathic pain following peripheral nerve injury has an obligation to refer to pain management when the post-injury pain is not responding to standard analgesic management within a clinically appropriate timeframe. Delayed referral is a standard of care concern when a patient with documented peripheral nerve injury and persistent neuropathic pain is managed for an extended period without pain management specialist involvement.
- › Appropriate pharmacological management — Opioid-centric management of peripheral neuropathic pain, without adequate trials of neuropathic-specific agents, is inconsistent with the current standard of care. The pain management record should document that appropriate neuropathic agents were offered, the patient's response to each agent, and the rationale for any treatment changes before escalating to higher-risk or higher-cost interventions.
- › Neuroma recognition and management — When a patient with peripheral nerve injury reports point-specific pain at the injury site that is exquisitely tender to palpation and worsened by mechanical provocation, the treating physician should recognize neuroma formation as a potential contributor and address it specifically — rather than attributing all pain to generalized neuropathic mechanisms. Failure to recognize and address a symptomatic neuroma may result in unnecessary escalation to systemic pharmacological or interventional treatments that do not address the actual pain generator.
Common Litigation Issues
Peripheral nerve injury cases present a defined set of recurring litigation issues across personal injury and malpractice contexts:
- › Diagnosis confirmation — Whether the peripheral nerve injury diagnosis is supported by the clinical and electrodiagnostic record. Defense review frequently addresses whether the electrodiagnostic study was technically adequate, whether the nerve survey was complete, whether the interpretation was correct, and whether alternative diagnoses — radiculopathy, psychogenic pain, or pre-existing neuropathy — could explain the findings.
- › Causation — Whether the alleged peripheral nerve injury is attributable to the subject event or to a pre-existing or subsequent cause. Pre-existing diabetic neuropathy, prior nerve entrapment, or prior injuries to the same nerve territory are common alternative causation arguments. Expert review addresses whether the electrodiagnostic findings are consistent with the mechanism, timing, and distribution of the alleged injury, and whether pre-existing conditions explain the findings.
- › Injury grade and prognosis disputes — Whether the injury is neuropraxia (expected full recovery), axonotmesis (partial recovery expected), or neurotmesis (no spontaneous recovery, surgery required) affects the prognosis, the expected treatment course, and the future care projections. Defense review often argues that the injury was neuropraxia with complete expected recovery — negating future care projections — when the plaintiff's expert characterizes it as axonotmesis or neurotmesis.
- › CRPS Type II development — Whether a peripheral nerve injury has progressed to CRPS Type II is a significant issue because the CRPS diagnosis substantially elevates the damages trajectory. Defense review often contests the CRPS Type II diagnosis on the grounds that the Budapest Criteria documentation is inadequate, that autonomic and trophic findings are absent or inconsistently documented, or that the treating physician applied the diagnosis without meeting the clinical criteria.
- › Medical necessity of treatment — Whether the volume, frequency, and type of treatment rendered is consistent with the documented injury severity and clinical course. Insurers and defense counsel frequently dispute the necessity of extended interventional treatment or the threshold for SCS escalation in peripheral nerve injury cases.
- › Future care projections — Whether SCS, ongoing pharmacological management, and other future care items in a plaintiff's life care plan are clinically supported by the documented injury severity and treatment course. Defense review addresses whether the projected care is medically indicated given the actual electrodiagnostic findings, whether SCS is a reasonable projection when conservative management has not yet been exhausted, and whether projected costs reflect current market pricing.
Personal Injury Analysis
Motor vehicle collisions, pedestrian incidents, slip-and-fall events, and machinery-related accidents are common personal injury mechanisms for peripheral nerve injury. High-energy mechanisms producing upper or lower extremity trauma — crush, laceration, or fracture — frequently involve peripheral nerve injury as a component of the overall traumatic picture. In personal injury matters, the causation analysis addresses whether the subject accident produced the nerve injury documented in the electrodiagnostic record, and whether the progression to CRPS Type II or refractory neuropathic pain requiring advanced treatment is a foreseeable consequence of that nerve injury. Expert review is most useful when the treating record contains serial electrodiagnostic studies that document the injury timeline, the degree of recovery, and the current nerve function status.
When a pre-existing neuropathic condition or degenerative process is present alongside the acute nerve injury, the causation analysis must distinguish incident-related change from natural disease progression; for the physician methodology governing that aggravation analysis, see the article on pre-existing degeneration vs. aggravation in spine injury cases.
Amputation cases — whether from traumatic amputation or from surgical amputation following vascular or traumatic injury — involve peripheral nerve injury as a component of the clinical picture. The nerves severed at amputation form neuromas at the residual limb; the pre-amputation peripheral nerve injury history affects the phantom limb pain trajectory; and the future care projections for an amputee with refractory pain must address both residual limb pain management and phantom limb pain management as distinct treatment needs. Expert review in amputation cases addresses the peripheral nerve injury and phantom limb pain components separately to provide a complete future care picture.
Medical Malpractice Analysis
Malpractice review in peripheral nerve injury cases arising from pain management — rather than from the surgical event itself — addresses whether the post-injury pain management met the applicable standard of care. This is a distinct question from the surgical standard of care, which addresses whether the nerve injury resulted from negligent surgical technique and requires a surgical expert.
- › Failure to diagnose or refer following surgical nerve injury — When a patient develops neuropathic pain in a peripheral nerve distribution following surgery, the surgeon has an obligation to recognize the possibility of intraoperative nerve injury and to refer to pain management or neurology when the symptoms persist beyond the expected recovery window. Delayed recognition and delayed referral are common standard of care issues in surgical nerve injury cases where the patient subsequently develops CRPS Type II or refractory neuropathic pain.
- › Failure to obtain electrodiagnostic evaluation — A pain management physician who assumes care of a patient with post-traumatic or post-surgical neuropathic pain without obtaining or reviewing electrodiagnostic studies when they are clinically indicated is not meeting the evaluation standard for peripheral nerve injury assessment. The treating physician cannot characterize the injury grade, the prognosis, or the appropriate treatment pathway without electrodiagnostic data, and proceeding to treatment without this foundational evaluation is a standard of care concern.
- › Failure to diagnose CRPS Type II — When a patient with confirmed peripheral nerve injury presents with disproportionate neuropathic pain, allodynia, and autonomic or trophic changes consistent with Budapest Criteria categories, failing to apply the CRPS Type II diagnosis — and failing to initiate CRPS-specific treatment, including timely sympathetic interventions and physical therapy — may constitute a departure from the standard of care, particularly given the evidence that early treatment affects long-term outcomes in CRPS.
- › Pain management standard of care in surgical nerve injury cases — These cases require careful delineation of the expert's scope. The surgical standard of care requires a surgeon expert. The pain management standard of care — how the post-injury neuropathic pain was evaluated and managed — requires a pain management expert. These are separate opinions, often from separate experts, and the retaining attorney should clarify at the outset which standard of care is the subject of the engagement.
Future Medical Care Review
Future medical care projections for peripheral nerve injury must be grounded in the documented injury grade, the current clinical and electrodiagnostic status, and the treatment course to date. The specific care items projected and their frequencies should reflect the actual trajectory documented in the medical record rather than generic template assumptions for a particular diagnosis.
- › Pharmacological management — Ongoing neuropathic agent prescriptions, with current dosing and market pricing, for patients whose current treatment includes pharmacological management with documented benefit. Projected medications should reflect those with documented clinical response in the current treating record, not speculative future agents.
- › Targeted nerve procedures — Perineural injections, nerve hydrodissection, or targeted block procedures that have been part of the treating course and are projected to continue based on the treating physician's plan and clinical trajectory. The frequency and cost of each procedure should be based on the documented treatment history and the current care plan.
- › Surgical intervention — Where neuroma excision, nerve grafting, or neurosurgical repair has been recommended by a treating physician, the cost of the anticipated procedure and its post-operative pain management needs is a recognized future care component. The clinical basis for the surgical recommendation — and the expected outcome — should be addressed in the projecting physician's opinion.
- › Spinal cord stimulation — Where the clinical record and current treatment trajectory support a future SCS need, the projection should include the trial procedure, permanent implantation with device-specific cost documentation, battery replacement cycles at published intervals, revision procedures at published complication rates, and ongoing programming visits. The clinical basis for projecting SCS — documented conservative care failure, appropriate indication, and a pain pattern consistent with SCS efficacy — must be addressed before including it as a future care item.
- › CRPS Type II future care — If CRPS Type II has developed from the peripheral nerve injury, the future care projection expands to include the full CRPS treatment trajectory — sympathetic nerve blocks, physical and occupational therapy, SCS — consistent with the CRPS literature and the patient's current clinical status. The CRPS Type II future care scope is materially broader than peripheral nerve injury alone and should be addressed as a distinct component when both diagnoses are present.
Future medical care review for peripheral nerve injury cases can be structured as a standalone engagement or combined with causation analysis. For California-specific matters, see the California Pain Management Expert Witness page.
Expert Witness Review Process
A complete expert review in a peripheral nerve injury case requires a defined set of records. The specific records needed depend on whether the engagement addresses causation, medical necessity, standard of care, or future care — or a combination defined in consultation with retaining counsel. Typical records include:
- › Electrodiagnostic records — All EMG and NCS studies performed in relation to the claimed nerve injury, with both the raw data and the interpreting physician's report; serial studies where available to document the injury timeline and recovery course
- › Treating pain management records — Complete notes from the initial pain management evaluation through the most recent encounter, documenting clinical findings, treatment administered, and patient response to each treatment modality
- › Initial treating records — Emergency department, urgent care, and initial physician records from the period immediately following the traumatic event or surgical procedure, documenting the clinical presentation at the earliest point
- › Surgical records (where applicable) — Operative reports from any surgical procedure alleged to have caused or been related to the nerve injury, anesthesia records, and pre- and post-operative clinical notes
- › Imaging — MRI studies of the affected nerve distribution or adjacent spinal levels; ultrasound or MRI neurography where obtained; X-rays documenting any associated bony injuries
- › Physical and occupational therapy records — Rehabilitation documentation from the post-injury period, documenting treatment approach, patient participation, and functional outcome measures
- › Prior medical records — Pre-injury records relevant to baseline nerve function, prior injuries to the same nerve distribution, and any pre-existing medical conditions that could affect the electrodiagnostic findings or the interpretation of the current clinical presentation
- › SCS-related records (where applicable) — Pre-implant psychological evaluation, trial stimulation documentation with pre- and post-trial pain scores, permanent implant records, and post-implant programming and follow-up notes
- › Deposition testimony — Testimony of the treating pain management physician, the operative surgeon (where surgical nerve injury is alleged), and any retained experts; claimant testimony on symptom history and functional limitations
Contact Expert Medical Services LLC with a brief case summary, a description of available records, and the specific questions to be addressed. Engagements covering causation, standard of care, and future medical care can be structured separately or together within a single retention.
Related Services & Expertise
CRPS Expert Witness
CRPS Type II follows confirmed peripheral nerve injury — diagnosis, Budapest Criteria, causation, and future care.
Spinal Cord Stimulation
SCS for refractory peripheral neuropathic pain — medical necessity, cost projections, and expert testimony.
Amputation & Phantom Limb Pain
Peripheral nerve injury, neuroma formation, and phantom limb pain overlap in complex amputation matters.
Post-Laminectomy Syndrome
Post-surgical neuropathic pain and nerve root injury following spinal surgery.
Future Medical Care Review
Long-term cost projections for neuropathic pain management, SCS, and peripheral nerve treatment.
Causation Analysis
Linking the traumatic mechanism to peripheral nerve injury diagnosis and treatment.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California nerve injury matters.
Independent Medical Evaluation
Structured examination to evaluate nerve injury, functional status, and treatment needs.
Arizona Pain Management Expert Witness
Peripheral nerve injury expert review for Arizona personal injury and malpractice litigation.
Medical Necessity Review
Medical necessity review for peripheral nerve injury treatment — neuromodulation candidacy and procedural justification.
Standard of Care Analysis
Standard of care analysis for peripheral nerve injury diagnosis, workup, and interventional pain management.
FAQ
Peripheral Nerve Injury — Common Attorney Questions
- Peripheral nerve injury refers to damage to nerves outside the central nervous system — the brain and spinal cord. The peripheral nervous system includes the motor and sensory nerves that carry signals between the central nervous system and the muscles, skin, and organs. Damage to these nerves produces neuropathic pain — burning, shooting, or electric quality pain that may include allodynia (pain from normally non-painful stimuli such as light touch or clothing contact) and hyperalgesia (exaggerated pain responses) — as well as sensory loss, weakness, or motor deficit in the distribution of the affected nerve. Peripheral nerve injury arises in the litigation context from traumatic mechanisms including lacerations, crush injuries, traction, and compression; from surgical complications in which a peripheral nerve is damaged during an operative procedure; and from entrapment or repetitive occupational exposure. The severity and prognosis depend on the mechanism and the degree of structural disruption to the nerve.
- Peripheral nerve injuries are classified using two overlapping systems — the Seddon classification (three grades) and the more detailed Sunderland system (five degrees). In the Seddon system: neuropraxia is the mildest injury, involving disruption of conduction without structural axon damage, with full recovery expected over weeks to a few months; axonotmesis involves disruption of the axon itself but preservation of the surrounding connective tissue structures (endoneurium, perineurium, epineurium), allowing axonal regrowth along the intact connective tissue scaffold at approximately 1–3 mm per day; and neurotmesis is complete nerve transection — both the axon and the surrounding connective tissue framework are disrupted — which typically requires surgical repair and carries the worst prognosis for functional recovery. The classification has direct clinical and medico-legal significance: it informs the prognosis for recovery, the appropriateness of surgical versus conservative management, and the expected timeline for electrodiagnostic evidence of reinnervation. Expert review addresses whether the treating documentation reflects a correct assessment of injury grade and an appropriate treatment approach matched to the classification.
- Electromyography (EMG) and nerve conduction studies (NCS) provide objective, physiological data on peripheral nerve function and are the primary diagnostic tools for confirming and characterizing peripheral nerve injury. Nerve conduction studies measure the speed (conduction velocity) and amplitude of electrical signals through a nerve, and can identify demyelination (slowing of conduction velocity), axon loss (reduction in signal amplitude), or conduction block at a specific location along the nerve. EMG evaluates the electrical activity of muscles at rest and during voluntary contraction, providing evidence of denervation (active injury) or reinnervation (recovery) in muscles supplied by the affected nerve. Together, NCS and EMG can confirm the diagnosis of peripheral nerve injury, identify the specific nerve involved, localize the injury along the nerve, grade its severity, and track recovery over serial studies. In the medico-legal context, the quality of the electrodiagnostic study — including the technical adequacy of the methodology, the completeness of the nerve survey, and the correlation between electrodiagnostic findings and the clinical presentation — is a central issue in both diagnosis confirmation and causation analysis.
- Causation review in peripheral nerve injury cases addresses whether the subject traumatic event produced the documented nerve injury. The analysis considers the mechanism of injury and its anatomical consistency with the nerve distribution affected — for example, a crush injury to the forearm that produces median or ulnar nerve findings on NCS is mechanistically consistent in a way that requires analysis of the forces, anatomy, and clinical timeline. The temporal relationship between the traumatic event and the onset of symptoms is assessed against the expected clinical course for the type of nerve injury proposed — neuropraxia should produce immediate or very early symptoms; axonotmesis and neurotmesis may produce immediate symptoms, but electrodiagnostic evidence of denervation typically does not appear until 10–21 days post-injury. The pre-existing medical history is reviewed to evaluate whether any pre-existing neuropathic condition, entrapment neuropathy, or prior nerve injury could explain the clinical and electrodiagnostic findings. Causation review is specific to pain management, and does not address surgical technique or the standard of care for neurosurgical repair — those require a separate expert.
- CRPS Type II — historically called causalgia — specifically requires a confirmed peripheral nerve injury and produces the full Complex Regional Pain Syndrome clinical picture in a distribution corresponding to the injured nerve. The diagnosis requires meeting the Budapest Criteria (documented symptoms in at least three of four clinical categories, with objective signs in at least two) with a confirmed nerve injury in the history or on electrodiagnostic testing. CRPS Type I, by contrast, occurs without a confirmed peripheral nerve injury; the precipitating event may be a fracture, sprain, contusion, or other injury. In peripheral nerve injury litigation, the distinction matters because: (1) a treating physician who fails to obtain electrodiagnostic studies when a peripheral nerve injury is clinically suspected may have missed a Type II diagnosis; (2) the presence or absence of a confirmed nerve injury affects the causation analysis; and (3) CRPS Type II arising from a confirmed surgical nerve injury can elevate a nerve injury case into a CRPS malpractice matter with materially different damages implications.
- A traumatic neuroma is a disorganized proliferation of nerve fiber and scar tissue that forms at the proximal end of a severed or severely injured peripheral nerve when nerve regeneration is blocked or misdirected. Neuromas are not benign in the clinical sense — they are highly sensitive, painful, and can produce severe local pain triggered by pressure, vibration, or movement, as well as radiating neuropathic pain in the distribution of the injured nerve. Traumatic neuromas arise from lacerations, crush injuries, or any mechanism that completely or near-completely severs a peripheral nerve. Surgical neuromas arise as a complication of procedures in which a peripheral nerve is cut, either intentionally (as in an amputation) or inadvertently (as a surgical complication). In litigation, neuromas arise in personal injury matters where a laceration or crush injury has produced chronic neuropathic pain that has not responded to conservative management, in amputation cases where the residual limb pain has a neuroma as a contributing component, and in malpractice matters where an inadvertent surgical nerve injury and subsequent neuroma formation are alleged.
- Spinal cord stimulation is considered for peripheral neuropathic pain — including pain from traumatic nerve injury, surgical nerve injury, and neuroma-related pain — when the pain is refractory to an adequate trial of conservative and conventional management. The evidence base for SCS in peripheral neuropathic pain is secondary to the evidence base for CRPS and post-laminectomy syndrome, but SCS is an established treatment option for refractory peripheral neuropathic pain of any etiology when the distribution and quality of pain is consistent with the dermatomal or peripheral nerve territory amenable to SCS lead coverage. In cases where the neuropathic pain involves a discrete peripheral nerve territory, peripheral nerve stimulation — direct stimulation of the injured nerve — may be considered as an alternative or adjunct to spinal cord stimulation. Medical necessity review for SCS in peripheral nerve injury cases addresses whether the specific pain pattern is appropriate for the modality, whether adequate conservative care has been documented, and whether the pre-implant evaluation sequence has been completed.
- The standard of care for peripheral nerve injury pain management addresses the obligations of the pain management physician who evaluates and treats a patient with neuropathic pain from a documented or suspected peripheral nerve injury. Core elements include: obtaining or reviewing available electrodiagnostic studies before initiating treatment — or ordering them when they have not been performed and the clinical picture suggests peripheral nerve involvement; correlating electrodiagnostic findings with the clinical presentation to confirm the diagnosis; implementing pharmacological management appropriate to neuropathic pain (calcium channel modulators, SNRIs, tricyclics) before escalating to interventional procedures; and recognizing when the pain pattern is consistent with CRPS Type II and applying the Budapest Criteria framework to the clinical evaluation. Failure to obtain electrodiagnostic evaluation when a peripheral nerve injury is clinically suspected, or failure to recognize and address CRPS Type II as a complication of peripheral nerve injury, are both documented standard of care concerns.
- Amputation and peripheral nerve injury overlap in several medico-legally significant ways. First, the peripheral nerves that are severed at the time of amputation form neuromas at the cut nerve ends — these neuromas contribute to residual limb pain and are a component of post-amputation pain that requires distinct management from phantom limb pain. Second, the pre-amputation peripheral nerve injury — whether from the traumatic mechanism that led to amputation or from vascular compromise — affects the character of post-amputation neuropathic pain and the trajectory of phantom limb pain. Third, spinal cord stimulation and peripheral nerve stimulation are recognized options for both phantom limb pain and refractory neuroma pain, creating an overlap between peripheral nerve injury, amputation, and neuromodulation future care projections. Expert review in complex amputation cases may need to address both peripheral nerve injury and phantom limb pain as distinct components of the ongoing pain syndrome.
- Yes. Dr. Dardashti accepts peripheral nerve injury engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides. Review is available for causation analysis, electrodiagnostic interpretation, standard of care review, and future medical care projections — or for a defined subset of those issues based on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain Dr. Dardashti for a Peripheral Nerve Injury Case
Dr. Dardashti accepts peripheral nerve injury engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.