Nationwide Pain & Injury Medical Expert Witness
Epidural Steroid Injection Expert Witness
Expert evaluation of epidural steroid injections in personal injury and medical malpractice — medical necessity, standard of care, causation of radicular pain, procedural complications, and future medical care projections.
Request AvailabilityCredentials & Qualifications
- Topic
- Epidural Steroid Injection (ESI)
- Also Known As
- Interlaminar, Transforaminal, Caudal ESI
- Specialty
- Interventional Pain Management
- Evaluation Areas
- Medical Necessity, Standard of Care, Causation, Future Care
- Review Scope
- Medical-Legal Review
- Testimony
- State & Federal Courts
Epidural Steroid Injections in Medical-Legal Review
Epidural steroid injections are among the most commonly performed interventional pain procedures in the United States — and among the most frequently scrutinized in personal injury litigation and medical malpractice review. Their high volume of utilization, the significant costs they generate, their role as a prerequisite for treatment escalation decisions, and the serious complications that can occur when performed incorrectly all make ESI a recurring subject of medical-legal dispute.
In personal injury matters, ESI arises when a traumatic event — a motor vehicle collision, workplace injury, or fall — produces disc herniation or nerve root compression requiring interventional treatment. The core disputes address whether each injection was medically necessary given the documented clinical findings, whether the number of injections performed was appropriate, and what future injection costs should be projected as part of damages. In medical malpractice matters, disputes address whether each injection was performed within the applicable standard of care, whether complications resulted from a procedural deviation, and whether the physician appropriately selected the approach, level, and medication type.
Expert review is grounded in the clinical and procedural record, the available imaging, and the scope of questions defined by retaining counsel. Opinions address pain management and interventional procedure standard of care — they do not address neurosurgical or orthopedic surgical standard of care.
What Is an Epidural Steroid Injection?
An epidural steroid injection delivers corticosteroid — typically combined with local anesthetic — into the epidural space of the spinal canal. The epidural space surrounds the dural sac and the nerve roots emerging from it, positioned between the ligamentum flavum posteriorly and the dura mater anteriorly. By depositing anti-inflammatory medication adjacent to an inflamed or compressed nerve root, ESI addresses the neurogenic inflammation that produces radicular pain — the shooting or burning pain that radiates from the spine into the extremity in a dermatomal pattern.
ESI is a symptomatic, anti-inflammatory treatment. It does not alter the structural pathology — it does not remove disc herniation material, widen a stenotic foramen, or decompress the spinal canal. Its clinical benefit is to reduce the inflammatory component of radicular pain, improve short- to medium-term function, and facilitate participation in physical therapy. It is appropriate for radicular pain with a documented structural correlate on imaging; it is not appropriate as a primary treatment for axial spine pain, facet-mediated pain, or pain without a radicular component.
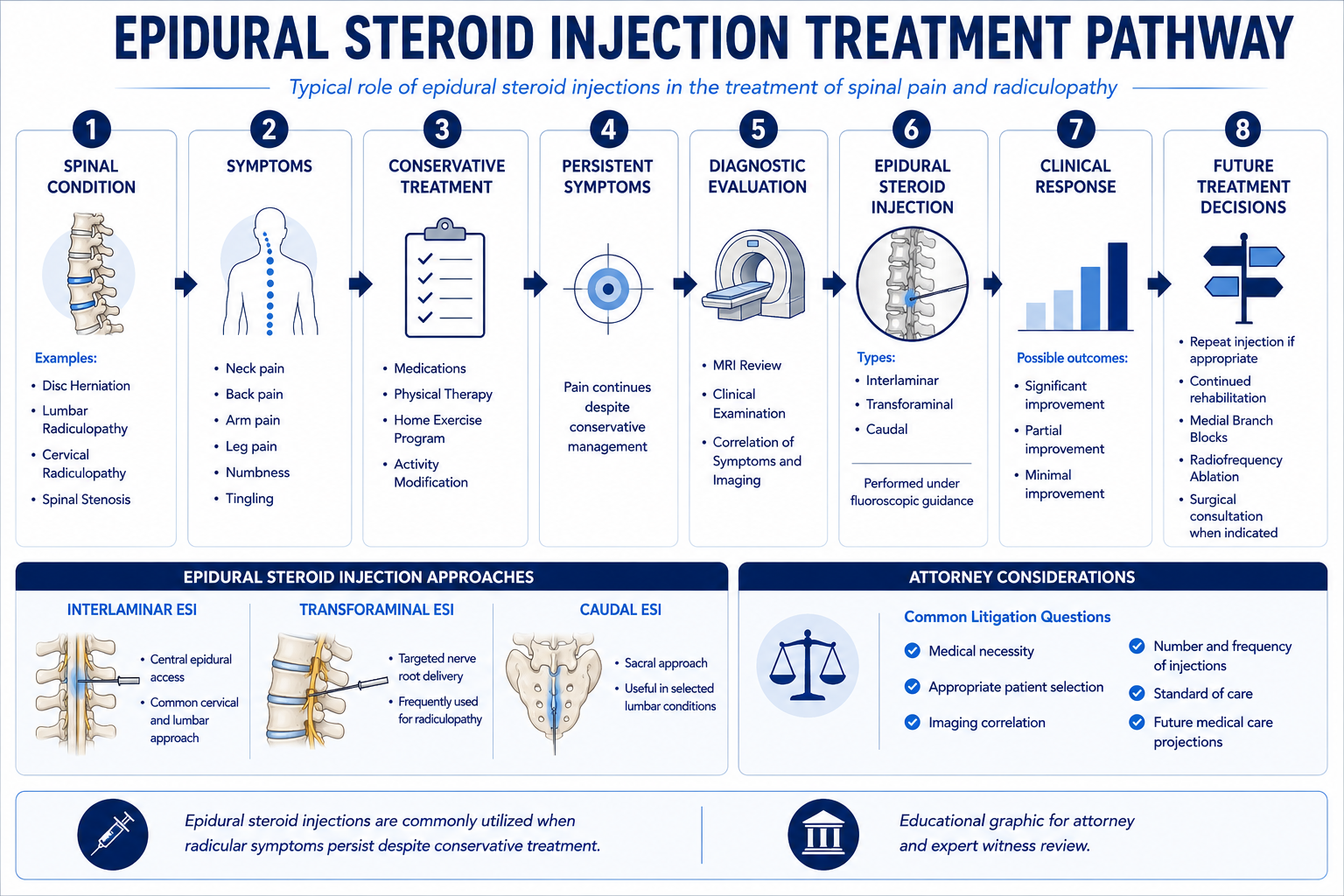
Three anatomical approaches are used depending on the clinical indication, the spinal level, and patient anatomy:
- › Interlaminar ESI — The needle is advanced through the ligamentum flavum in the posterior midline or paramedian position to enter the epidural space at the level of the target nerve root. Interlaminar ESI distributes medication broadly within the epidural space and provides bilateral coverage. It is technically more accessible at most lumbar and cervical levels and is the preferred approach for bilateral radicular pain or when targeted unilateral delivery is not required. The primary risk specific to interlaminar ESI — versus transforaminal — is inadvertent dural puncture with the needle, which can produce a post-dural puncture headache from cerebrospinal fluid leak. At the cervical level, interlaminar ESI carries additional considerations related to spinal cord proximity, and fluoroscopic guidance with contrast confirmation of epidural spread is particularly important.
- › Transforaminal ESI — The needle is directed through the neural foramen to position the tip in the anterior epidural space immediately adjacent to the exiting nerve root and the posterior disc — the site where disc herniation material most directly contacts and inflames the nerve root. Transforaminal ESI provides the most targeted delivery of medication to the precise anatomical site of nerve root irritation and is the preferred approach for unilateral single-level radiculopathy when a specific nerve root is identified on imaging as the pain generator. The primary safety consideration unique to transforaminal ESI involves the radicular artery that runs with the nerve root in the foramen — inadvertent intravascular injection into this artery carries a risk of embolic stroke, and particulate corticosteroid formulations (triamcinolone) at cervical levels pose an elevated embolic risk. Published society guidelines and FDA warnings recommend non-particulate steroids for cervical transforaminal ESI specifically because of this risk, and the use of particulate steroids for cervical transforaminal injections is a recognized standard of care issue in cervical ESI malpractice cases.
- › Caudal ESI — The needle enters the epidural space through the sacral hiatus at the base of the sacrum. Caudal injection accesses the epidural space from below and distributes medication through the sacral and lower lumbar epidural space when positioned with adequate volume. It is used for lower lumbar and sacral radicular pain, and is particularly useful when the lumbar epidural space is difficult to access interlaminar due to prior lumbar surgery, extensive epidural fibrosis, or calcified ligamentum flavum. In post-surgical lumbar pain patients, caudal ESI avoids the surgical field and associated scar tissue that can make interlaminar approaches technically challenging.
The selection of approach is a clinical decision based on the specific indication, the imaging findings, the patient's surgical history, and the anatomy. In medical necessity and standard of care review, the appropriateness of the selected approach for the documented clinical situation is subject to evaluation.
Common Indications
ESI is clinically appropriate for specific conditions producing nerve root compression or irritation with a documented radicular pain component. The primary recognized indications include:
- › Lumbar radiculopathy from disc herniation — The most common ESI indication. A lumbar disc herniation — most frequently at L4–L5 or L5–S1 — compresses or irritates the exiting nerve root, producing radicular pain that radiates from the low back into the leg in a dermatomal distribution. ESI is appropriate when the radicular pain has not responded to conservative management and imaging demonstrates disc herniation at the level and side corresponding to the clinical distribution. Transforaminal ESI at the affected level provides targeted anti-inflammatory delivery adjacent to the herniation-nerve root interface.
- › Cervical radiculopathy from disc herniation — A cervical disc herniation — most frequently at C5–C6 or C6–C7 — compresses the exiting nerve root in the foramen or at the posterior disc margin, producing radicular pain radiating into the shoulder, arm, forearm, or hand in the affected nerve root distribution. Cervical ESI is appropriate for cervical radiculopathy with imaging correlation when conservative management has not provided adequate relief. Cervical transforaminal ESI with non-particulate steroid is the preferred approach for unilateral single-level cervical radiculopathy; cervical interlaminar ESI addresses bilateral or multilevel cervical radicular pain.
- › Lumbar spinal stenosis with radicular pain — Degenerative lumbar stenosis — from a combination of disc bulging, facet hypertrophy, and ligamentum flavum thickening — narrows the central canal or lateral recesses, compressing nerve roots and producing neurogenic claudication (leg pain and weakness with walking that is relieved with sitting or forward flexion) and radicular pain. ESI for spinal stenosis addresses the inflammatory component of nerve root compression in a degenerating canal and may provide meaningful short-term functional improvement. The effect of ESI in stenosis is generally more modest and shorter-duration than in acute disc herniation, and the clinical record should document response to each injection before proceeding to additional procedures.
- › Post-surgical radicular pain — Patients with persistent radicular pain following spinal surgery — decompression, discectomy, or fusion — may benefit from ESI when the residual or recurrent radicular component reflects ongoing nerve root irritation rather than mechanical compression from epidural fibrosis or recurrent herniation. In the post-laminectomy syndrome context, ESI is one component of the interventional treatment ladder for post-surgical radicular pain, used before escalation to medial branch blocks for any facet component, and before consideration of spinal cord stimulation for refractory cases. The distinction between radicular pain amenable to ESI and axial mechanical or facet pain requiring medial branch blocks is a critical clinical decision that affects the appropriateness of ESI in the post-surgical patient.
- › Acute disc herniation with severe radicular pain — ESI may be used as a bridge treatment for acute severe disc herniation radiculopathy when the clinical situation is not immediately surgical, allowing the patient to participate in physical therapy and potentially defer or avoid surgery. In the personal injury context, acute post-traumatic disc herniation with severe radiculopathy is a recognized clinical situation in which early ESI may be both medically justified and strategically important to functional recovery.
ESI is generally not the appropriate treatment for axial back or neck pain without a radicular component; for pain attributed primarily to facet joints (which is addressed by medial branch blocks and radiofrequency ablation); for sacroiliac joint pain; or for pain that lacks imaging correlation with a structural cause. Performing ESI for pain that does not have a radicular character or a documented structural nerve root irritation cause is a medical necessity concern.
Medical Necessity Considerations
Medical necessity review for ESI addresses whether each injection was clinically appropriate based on the documented findings at the time the procedure was performed. The following elements constitute the standard necessity framework:
- › Documented radicular clinical findings — The clinical record should demonstrate radicular symptom characterization — specifically, pain radiating into the extremity in a nerve root distribution, with or without sensory changes or weakness in the affected territory. A clinical note describing only "back pain" or "neck pain" without a documented radicular component does not establish the primary indication for ESI. The physical examination should include assessment of dermatomal sensory changes, motor strength in the relevant muscle groups, and reflex changes in the affected extremity.
- › Imaging correlation — MRI or CT imaging should demonstrate a structural cause of nerve root compression or irritation — disc herniation, foraminal stenosis, or lateral recess stenosis — at the level and side corresponding to the patient's clinical pain distribution. Performing ESI at a level not supported by imaging, at a side not consistent with the clinical presentation, or for a pain distribution not correlated with any structural imaging finding is a medical necessity deficiency. The imaging report and the pre-procedure clinical note should be reviewed together to confirm that the level and side selected for injection match the documented clinical and imaging picture.
- › Conservative treatment requirements — Most clinical guidelines and payer policies require documentation of a trial of conservative management before ESI is authorized. Conservative management typically includes a combination of anti-inflammatory medications, activity modification, and physical therapy or chiropractic care. The duration and adequacy of the required conservative care trial varies by guideline and payer policy, but an ESI performed at the initial patient visit — before any conservative measures have been attempted — may face a necessity challenge absent a clinical justification for bypassing the conservative requirement (such as severe neurological deficit, intractable pain, or a history of prior failed conservative care).
- › Documented functional impairment — The clinical record should characterize the functional impact of the radicular pain — limitations in ambulation, work capacity, activities of daily living — to contextualize the necessity and urgency of intervention. Functional documentation also establishes the baseline against which the treatment response is assessed, which is relevant both to necessity review and to future care projections.
- › Documented response basis for repeat injections — The most important necessity element for each subsequent injection is documentation of the clinical response to the prior injection. The post-procedure note following each injection should document the percentage of pain relief achieved and the duration of relief, using a validated pain scale. This documentation is the clinical basis for the decision to repeat the injection. An injection performed on a patient who reported no meaningful relief from the prior injection — or for whom no post-procedure assessment was documented — does not meet the standard for an evidence-based repeat injection decision.
Standard of Care
The standard of care for ESI performance reflects the practice of a reasonably competent board-certified interventional pain management physician. Core technical and documentation elements include:
- › Fluoroscopic guidance — Real-time fluoroscopic imaging is required for all ESI approaches. Performing ESI without fluoroscopic guidance — a "blind" injection relying on tactile landmarks alone — is below the current standard of care for cervical ESI and is considered a deviation in most clinical and medicolegal contexts for lumbar ESI as well. Fluoroscopy confirms needle positioning before medication is injected, reducing the risk of dural puncture, intravascular injection, and medication delivery outside the epidural space.
- › Contrast injection for epidural and non-vascular confirmation — Before injecting corticosteroid, contrast medium should be injected under live fluoroscopy to confirm epidural spread of injectate and — critically — to confirm that the needle tip is not positioned intravascularly. An intravascular injection pattern on contrast imaging requires needle repositioning before proceeding. Injection of particulate steroid through a needle that has not been confirmed as non-intravascular is a recognized standard of care deviation and the primary mechanism of the most serious ESI complication — embolic stroke in cervical transforaminal ESI.
- › Steroid selection — cervical transforaminal procedures — FDA warnings and published society guidelines (including Spine Intervention Society and ASIPP guidelines) specifically address the use of particulate versus non-particulate corticosteroids for cervical transforaminal ESI. Particulate steroids — including triamcinolone — can aggregate into embolic particles if injected intravascularly and have been associated with catastrophic embolic stroke in the posterior circulation. The standard of care for cervical transforaminal ESI requires use of a non-particulate steroid — dexamethasone — to minimize this risk. Use of triamcinolone or methylprednisolone for cervical transforaminal injection is a standard of care issue in cervical ESI malpractice cases involving embolic complications.
- › Documentation requirements — The procedure report should document: the approach and level(s) treated; the needle type and gauge; the contrast agent used and the documented epidural spread pattern; the medications injected with doses; patient tolerance; and any intraoperative findings. Post-procedure monitoring before patient discharge should be documented. A procedure note that does not document contrast confirmation, the specific medications and doses administered, or the fluoroscopic findings is below the documentation standard for interventional pain procedures.
- › Patient selection and contraindication screening — Standard pre-procedure evaluation should include review of anticoagulation status — patients on anticoagulants require specific management consistent with published guidelines for the type of anticoagulant and the procedure approach. Coagulopathy, active infection, and allergy to procedure medications are contraindications that must be assessed and documented. Proceeding to ESI in an anticoagulated patient without appropriate anticoagulation management is a recognized standard of care issue.
- › Informed consent — Consent should address the specific risks of the approach to be performed — including dural puncture, infection, bleeding, nerve injury, and in cervical procedures, the specific embolic risk — as well as the expected benefit profile and the alternatives. An inadequate or absent consent process is a standard of care issue in complication cases where the patient alleges lack of informed consent about the specific complication that occurred.
Common Litigation Issues
ESI-related disputes in personal injury and malpractice litigation fall into several recurring categories:
- › Medical necessity disputes — The most common ESI litigation issue. Defense and insurer review challenges whether each injection was individually supported by a documented radicular indication, imaging correlation with the treated level and side, and adequate documentation of response to prior injections before repeating the procedure. High-volume ESI series — six, eight, or ten or more injections — are particularly subject to necessity scrutiny when the clinical record does not contain contemporaneous post-procedure response documentation for each procedure.
- › Excessive procedure volume — When a treating physician performs substantially more ESIs per year than clinical guidelines support, or performs multiple injections per spinal region at rates exceeding the published safety and effectiveness evidence, the excess procedures above a clinically supported number may be contested for both past and future care purposes. Expert review addresses what number of injections is supported by the clinical record, what guidelines apply, and what the excess volume represents in terms of billed charges.
- › Wrong-level or wrong-side injections — ESI performed at a level not supported by the imaging, at a side contralateral to the documented disc herniation, or without any imaging correlation is a medical necessity and standard of care issue. Wrong-level injection claims may also arise in the malpractice context when an injection at an incorrect level produces an adverse outcome, though wrong-level injections are more commonly an issue in RFA than in ESI.
- › Documentation deficiencies — Missing, incomplete, or template-based procedure documentation that does not reflect the individual patient's procedure is a recurring issue. Identical or near-identical procedure notes across multiple procedures, absence of documented contrast confirmation, failure to document post-procedure response, or absence of pre-procedure consent documentation are all documentation-based challenges in ESI litigation. These deficiencies do not necessarily mean the procedure was performed incorrectly, but they undermine the clinical record's ability to support either necessity or standard of care positions.
- › Billing and coding disputes — CPT code selection for ESI — which varies by approach (interlaminar vs. transforaminal), spinal region (cervical/thoracic vs. lumbar/sacral), and number of levels — is a recurring source of billing disputes. Up-coding (billing for a more complex or more targeted approach than was performed), billing for bilateral procedures when only unilateral injection was documented, and unbundling of related services are billing accuracy issues distinct from clinical necessity or standard of care.
Personal Injury Analysis
Motor vehicle collisions are the most common personal injury mechanism producing disc herniation and radiculopathy requiring ESI. Rear-impact collisions produce a hyperextension-flexion mechanism in the cervical spine that can generate significant forces on the cervical discs and facet joints, and cervical disc herniation with radiculopathy is a well-documented injury type following high-energy rear-impact collisions. Frontal and lateral impacts produce different cervical loading patterns, and the mechanism analysis is specific to the collision geometry, the magnitude of the impact, and the patient's body position at the time of impact. Lumbar disc herniation from motor vehicle collision may follow axial compressive loading, rotational forces, or a combination mechanism.
Pre-existing degenerative spinal disease is among the most frequently contested issues in personal injury ESI cases. Disc degeneration and facet arthrosis are present in the majority of adults over forty and may be visible on imaging obtained after the accident. The defense frequently argues that the disc herniation requiring ESI was pre-existing and degenerative rather than traumatic — that the accident did not cause the disc pathology, but merely coincided with it. The causation analysis addresses this argument directly: the analysis considers whether the accident mechanism was sufficient to produce disc herniation at the documented level, whether the temporal relationship between the event and symptom onset is consistent with traumatic causation, and whether the imaging findings are more consistent with acute traumatic herniation versus chronic degenerative change.
Future ESI costs in personal injury cases should be grounded in the clinical trajectory and the treating physician's prognosis for the underlying condition. When the radicular pain is expected to require ongoing treatment — particularly in patients with spinal stenosis or multilevel degeneration where definitive surgical treatment is not pursued — a projected ESI series with documented frequency and duration is a recognized future care component. When the clinical trajectory supports eventual escalation to medial branch blocks and radiofrequency ablation, those escalation costs should be projected separately.
Medical Malpractice Analysis
Malpractice claims arising from ESI fall into two broad categories: complications attributable to procedural deviation, and harm attributable to inappropriate patient selection or inadequate pre-procedure evaluation. Expert review addresses whether the care met the standard of a reasonably competent board-certified interventional pain management physician. Adequate pre-procedure evaluation includes a documented physical examination with findings consistent with the clinical indication; for the complete objective evaluation methodology expected of a pain management physician, see the article on how pain management experts objectively evaluate pain.
- › Dural puncture and post-dural puncture headache — Inadvertent dural puncture during interlaminar ESI is a recognized procedural complication producing post-dural puncture headache — a severe positional headache caused by cerebrospinal fluid leak through the dural tear. It may be a recognized risk of the procedure rather than a standard of care deviation, depending on the clinical circumstances and technique. Malpractice analysis addresses whether the use of fluoroscopic guidance, appropriate needle selection, and correct technique was consistent with the standard, and whether the complication was recognized and managed appropriately after it occurred.
- › Epidural abscess and infection — Epidural abscess is a rare but catastrophic complication of ESI — an infection in the epidural space that can rapidly progress to spinal cord compression. Risk factors include diabetes, immunosuppression, and prior spinal surgery. Causation analysis in epidural abscess cases addresses whether the procedural technique included appropriate sterility measures, whether the patient had documented risk factors for infection that affected the risk-benefit calculation for the procedure, and whether the post-procedure clinical course was consistent with procedurally introduced infection versus community-acquired or hematogenous seeding.
- › Intravascular injection and embolic complications — The most serious ESI complications involve intravascular injection — particularly in cervical transforaminal procedures. Injection of particulate steroid through a needle positioned in the radicular artery or another epidural vessel can produce posterior circulation embolic stroke with devastating neurological consequences. Standard of care review addresses whether contrast confirmation was performed under live fluoroscopy to exclude intravascular positioning before steroid injection, whether a non-particulate steroid was used for cervical transforaminal injection consistent with published guidelines, and whether standard technique was followed to minimize intravascular injection risk.
- › Nerve injury — Direct nerve injury from needle contact with a nerve root during ESI can produce acute radicular pain at the time of injection — a warning sign that requires immediate needle withdrawal — and may result in lasting neuropathic pain or motor deficit. Standard of care review addresses whether the needle was advanced using appropriate incremental technique with intermittent fluoroscopic confirmation, and whether the appropriate response to intraprocedural radicular pain was taken.
- › Failure to follow accepted technique — Broader deviations from accepted technique — performing the procedure without fluoroscopy, injecting without contrast confirmation, using contraindicated medications, or failing to monitor appropriately — are all documented standard of care issues that may form the basis of malpractice claims when complications occur.
Future Medical Care Review
Future medical care projections for patients with radicular spinal pain treated with ESI should reflect the clinical trajectory documented in the treating record and the expected natural history of the underlying condition — not a maximum-frequency template for a given diagnosis. A defensible future ESI projection addresses:
- › Repeat injections — When the treating physician's clinical plan includes ongoing ESI and the condition is expected to persist based on imaging findings and clinical prognosis, repeat injections are a legitimate future care component. The projected frequency should be consistent with clinical guidelines (three to four per spinal region per year at most), the duration of projected need should be grounded in the treating physician's prognosis, and costs should reflect current geographic market pricing — not inflated retail rates or bundled facility-professional charges.
- › Escalation to medial branch blocks and radiofrequency ablation — When the clinical picture includes both radicular and facet-mediated components, or when the radicular pain responds to ESI but axial pain does not, escalation to medial branch blocks and ultimately radiofrequency ablation may be a reasonable future care projection. MBB and RFA constitute separate and distinct costs from ESI and should be projected separately with their own clinical basis and cost documentation.
- › Escalation to spinal cord stimulation — When the clinical trajectory includes refractory radicular neuropathic pain that is expected to persist beyond the period addressed by ESI and other conventional interventional management — particularly in post-laminectomy syndrome patients with persistent radicular pain — escalation to spinal cord stimulation may be a future care projection with independent cost components. The clinical basis for projecting SCS — documented ESI failure, appropriate indication, adequate conservative care trial — must be addressed separately from the ESI projection.
- › Defense review of future ESI projections — Defense review addresses whether the projected injection frequency exceeds clinical guidelines, whether the clinical record supports ongoing ESI need (as opposed to a patient who should have responded to conservative management by the time of trial), whether the underlying structural condition is likely to require surgical treatment that would eliminate the need for further injection management, and whether projected costs reflect current market pricing.
Expert Witness Review Process
A complete expert review in an ESI case requires a defined record set. The specific records depend on whether the engagement addresses medical necessity, standard of care for procedure performance, causation of the underlying radicular condition, or future care projections — or a combination. Typical records include:
- › Treating pain management records — Complete records from initial evaluation through the most recent encounter, including initial history and physical, follow-up notes, pre-procedure assessments for each injection, procedure reports, post-procedure response documentation, and pharmacological management notes
- › Procedure reports and fluoroscopy documentation — Individual procedure reports for each ESI performed, documenting the approach, level, needle type, contrast confirmation pattern, medications injected with doses, and patient tolerance; fluoroscopy images or fluoroscopy record where available
- › Post-procedure response documentation — Clinical notes or pain diary records documenting the percentage and duration of pain relief following each injection — the primary clinical basis for the decision to repeat or escalate treatment; absence of these records is itself a significant finding in necessity review
- › Imaging studies — MRI of the relevant spinal region (cervical or lumbar) with radiology report, correlating imaging findings with the clinical pain distribution and the levels and sides treated; any post-surgical imaging where prior spinal surgery is relevant
- › Billing records — Itemized billing by CPT code and date of service for all procedures and visits; authorization records and payer correspondence where insurance disputes are at issue
- › Initial treating records — Emergency department, urgent care, primary care, and chiropractic records from the period immediately following the traumatic event through the first pain management evaluation, documenting symptom onset, initial clinical findings, and conservative care provided
- › Prior treating records — Records predating the subject event establishing baseline spinal health, prior episodes of back or radicular pain, prior imaging, and any prior injections at the same levels
- › Physical therapy and chiropractic records — Documentation of the conservative care provided before and concurrent with ESI treatment; relevant to both the adequacy of the conservative care trial and the functional improvement documentation
- › Deposition testimony — Treating pain management physician testimony addressing clinical rationale, procedure selection, and patient-reported response; claimant testimony on symptom history and functional limitations
Contact Expert Medical Services LLC with a brief case summary, a description of the available records, and the specific questions to be addressed. Engagements can be structured to address medical necessity, standard of care, causation, and future medical care separately or together within a single retention. For California-specific matters, see the California Pain Management Expert Witness page.
Related Services & Expertise
Medial Branch Block
MBB for facet-mediated axial pain — the distinct interventional pathway when ESI is not the appropriate treatment.
Radiofrequency Ablation
RFA for longer-duration facet pain relief — the escalation pathway when MBB confirms facet-mediated pain.
Post-Laminectomy Syndrome
Post-surgical radicular pain — a recognized ESI indication following spinal decompression or fusion surgery.
Spinal Cord Stimulation
SCS when ESI and conventional management fail — medical necessity, cost projections, and expert testimony.
CRPS Expert Witness
CRPS may develop after spinal injury and surgery — sympathetic blocks and SCS as escalation from ESI.
Future Medical Care Review
Projecting ongoing ESI, MBB/RFA, and escalation costs for personal injury damages analysis.
Causation Analysis
Linking the traumatic mechanism to disc herniation and the need for epidural steroid injection.
Expert Witness — California
Full-scope expert testimony for trial, deposition, and arbitration in California ESI matters.
Arizona Pain Management Expert Witness
Epidural steroid injection expert review for Arizona personal injury and malpractice litigation.
Independent Medical Evaluation
Structured IME with written opinion for cases requiring direct examination alongside records review.
Medical Necessity Review
Medical necessity review for epidural steroid injections — frequency, imaging requirements, and fluoroscopic guidance standards.
Standard of Care Analysis
Standard of care analysis for epidural injection technique, documentation, and appropriate patient selection.
FAQ
Epidural Steroid Injections — Common Attorney Questions
- An epidural steroid injection (ESI) is a fluoroscopically guided interventional pain procedure in which corticosteroid — most commonly triamcinolone, methylprednisolone, or dexamethasone — combined with local anesthetic is delivered into the epidural space adjacent to an inflamed or compressed nerve root. The epidural space is the potential space between the ligamentum flavum and the dura mater within the spinal canal, and it surrounds the nerve roots as they travel toward their exit foramina. By delivering anti-inflammatory medication directly to the site of nerve root irritation, ESI aims to reduce neurogenic inflammation, decrease radicular pain, and improve functional capacity. ESI is not a structural treatment — it does not alter disc herniation, remove osteophytes, or decompress stenotic foramina. Its clinical benefit is anti-inflammatory and symptomatic, and it is appropriate for radicular pain with a documented structural cause rather than for axial mechanical or facet-mediated pain, which is addressed by different interventional approaches.
- The three ESI approaches differ in needle trajectory, anatomical target, and clinical appropriateness. The interlaminar approach delivers medication through the posterior or paramedian midline into the epidural space at the level of the target nerve root. It bathes the epidural space broadly and is appropriate for bilateral or multilevel radicular pain patterns, or when the transforaminal approach is not technically feasible. The transforaminal approach targets the medication delivery to the anterior epidural space immediately adjacent to the exiting nerve root at the neural foramen — the site where disc herniation material and inflammatory mediators most directly irritate the nerve root. Transforaminal ESI is generally preferred for unilateral single-level radiculopathy because it provides more targeted delivery to the precise site of nerve root inflammation. The caudal approach enters the epidural space through the sacral hiatus and is used primarily for lower lumbar and sacral radicular pain, particularly in patients with prior lumbar surgery where the lumbar epidural space may be difficult to access safely. Approach selection affects both the clinical appropriateness analysis and the standard of care review — choosing an approach that does not match the clinical indication or the anatomical situation may be subject to scrutiny.
- Medical necessity for ESI is generally supported by: (1) documented radicular pain — pain radiating in a dermatomal or nerve root distribution into the extremity, with or without sensory changes or weakness; (2) imaging evidence of a structural cause of nerve root compression or irritation consistent with the clinical distribution — disc herniation, foraminal stenosis, or lateral recess stenosis at the level and side corresponding to the symptoms; (3) failure of an adequate trial of conservative management — typically including anti-inflammatory medications, physical therapy, and activity modification; and (4) documented functional impairment from the radicular pain. ESI is not medically necessary for axial back or neck pain without a radicular component, for pain in a distribution that does not correspond to a structural finding on imaging, or when imaging does not demonstrate nerve root compression or irritation at a level and side consistent with the symptoms. In litigation, medical necessity disputes frequently center on whether the documented pain was genuinely radicular rather than axial, whether imaging findings supported the level and side treated, and whether adequate conservative management was completed before proceeding to injection.
- Most clinical guidelines — including those from professional societies and CMS coverage policies — limit epidural steroid injections to three to four procedures per spinal region per year, with some allowing up to six under specific circumstances. The clinical rationale for frequency limits is twofold: the total corticosteroid dose delivered by multiple injections can produce systemic effects including hypothalamic-pituitary-adrenal axis suppression; and epidural steroid injections that are not producing meaningful clinical benefit should not be repeated, but should prompt reassessment of the pain generator and consideration of alternative treatment. The decision to repeat an ESI should be based on documented meaningful relief from the prior injection. Repeating ESI in a patient who reported no relief from the previous injection — or in a patient who reported only axial back pain relief without radicular improvement — is a medical necessity concern. In litigation, a series of six to ten or more ESIs within a short period raises questions about whether each injection was individually supported by clinical indication and documented response.
- Causation review for ESI addresses whether the subject traumatic event — a motor vehicle collision, workplace injury, or fall — produced the disc herniation or nerve root compression that requires the injection. The analysis examines the temporal relationship between the event and the onset of radicular symptoms; the mechanism of injury and its anatomical consistency with the disc level involved; the pre-accident spinal history and any prior imaging or prior radicular symptoms; and the clinical documentation from the period between the accident and the first injection confirming the radicular character of the pain. In motor vehicle collisions, disc herniation from an acute compressive or torsional force is a recognized injury mechanism, but the defense commonly argues that the identified disc herniation is degenerative rather than traumatic — particularly when the patient has a history of prior back problems or when imaging shows multilevel degeneration. The causation analysis addresses whether the event produced new disc pathology, aggravated a symptomatic pre-existing disc condition, or accelerated an asymptomatic degenerative disc to become symptomatic.
- The standard of care for ESI performance requires: fluoroscopic guidance — real-time X-ray imaging to confirm needle position before injection; contrast injection to confirm epidural spread before steroid injection, specifically to verify that the needle tip is not intravascular (intravascular injection of particulate steroids carries a catastrophic risk of embolic stroke in certain approaches); proper patient positioning and informed consent; documentation of the procedure including needle approach, levels treated, contrast confirmation, medications injected, and patient tolerance; and post-procedure monitoring before patient discharge. Performing ESI without fluoroscopic guidance — also called a "blind" injection — is below the current standard of care and is a recognized source of complications including inadequate drug delivery, dural puncture, and intravascular injection. Performing a transforaminal ESI at a cervical level with particulate steroids — specifically using triamcinolone rather than a non-particulate steroid — carries an elevated risk of embolic stroke and is addressed in published FDA warnings and society guidelines. The use of particulate versus non-particulate steroids in cervical transforaminal ESI is a standard of care issue in cervical injection malpractice cases.
- Complications reviewed in ESI malpractice matters include: dural puncture — inadvertent puncture of the dura mater producing a post-dural puncture headache (spinal headache) from cerebrospinal fluid leak; epidural hematoma — accumulation of blood in the epidural space producing spinal cord or cauda equina compression, a surgical emergency; infection — epidural abscess from procedural contamination, particularly in patients with risk factors such as immunosuppression or diabetes; intravascular injection — injection of medication directly into an epidural vein or artery, carrying the risk of local anesthetic toxicity or, in cervical transforaminal procedures using particulate steroids, embolic stroke; nerve injury from direct needle trauma; and wrong-level treatment — injection at a level not supported by the clinical indication or not correlated with the imaging findings. Claims also arise from failure to obtain adequate consent addressing specific procedural risks, failure to document contraindications such as anticoagulation, and failure to monitor appropriately for post-procedure complications.
- Yes, when the clinical record supports ongoing radicular pain with an established indication for periodic ESI, future injection costs are a recognized component of personal injury damages analysis. A defensible future ESI projection requires: a clinical basis for expecting the radicular pain condition to persist — grounded in the clinical trajectory, imaging findings, and the treating physician's prognosis; a projected injection frequency consistent with clinical guidelines (typically no more than three to four per spinal region per year), not a maximum-frequency template; the current market cost of the procedure in the patient's geographic treatment area, including physician fees, facility fees, and fluoroscopy charges; and an assessment of whether the clinical trajectory supports eventual escalation from ESI to medial branch blocks, radiofrequency ablation, or spinal cord stimulation — each of which constitutes a separate and distinct future care cost component. Future ESI projections that assume maximum frequency indefinitely without addressing the clinical basis for that frequency are subject to challenge.
- Key records include: the complete treating pain management records from initial evaluation through the most recent encounter; procedure reports for each ESI performed documenting the approach, level, medications, fluoroscopy technique, contrast confirmation, and patient tolerance; post-procedure pain assessments documenting the percentage and duration of relief from each injection — these are the primary basis for establishing whether repeat injections were clinically supported; pre-procedure imaging (MRI of the relevant spinal segment with radiology report) correlating imaging findings with the treated level and side; billing records itemized by CPT code and date of service to establish the volume and frequency of procedures; insurance authorization records and payer correspondence; prior treating records predating the pain management relationship; and any functional capacity evaluation or physical therapy records documenting the functional limitations used to support the necessity of injection treatment.
- Yes. Dr. Dardashti accepts ESI engagements for plaintiff counsel, defense counsel, insurance defense, and medical malpractice matters for both sides. Review is available for medical necessity, standard of care, causation of the underlying radicular condition, and future medical care projections — or for a defined subset of those issues based on the questions retaining counsel needs addressed. Engagements are structured after a brief case summary is provided to confirm scope and availability.
Retain Dr. Dardashti for an Epidural Steroid Injection Case
Dr. Dardashti accepts ESI engagements for both retaining parties. Contact Expert Medical Services LLC to discuss case scope and availability.